

High-dose alkylating chemotherapy in BRCA-altered triple-negative breast cancer: the randomized phase III NeoTN trial
- PMID: 37689749
- PMCID: PMC10492793
- DOI: 10.1038/s41523-023-00580-9
High-dose alkylating chemotherapy in BRCA-altered triple-negative breast cancer: the randomized phase III NeoTN trial
Abstract
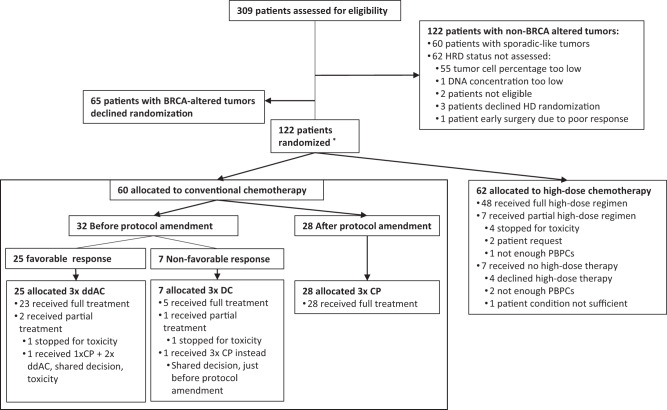
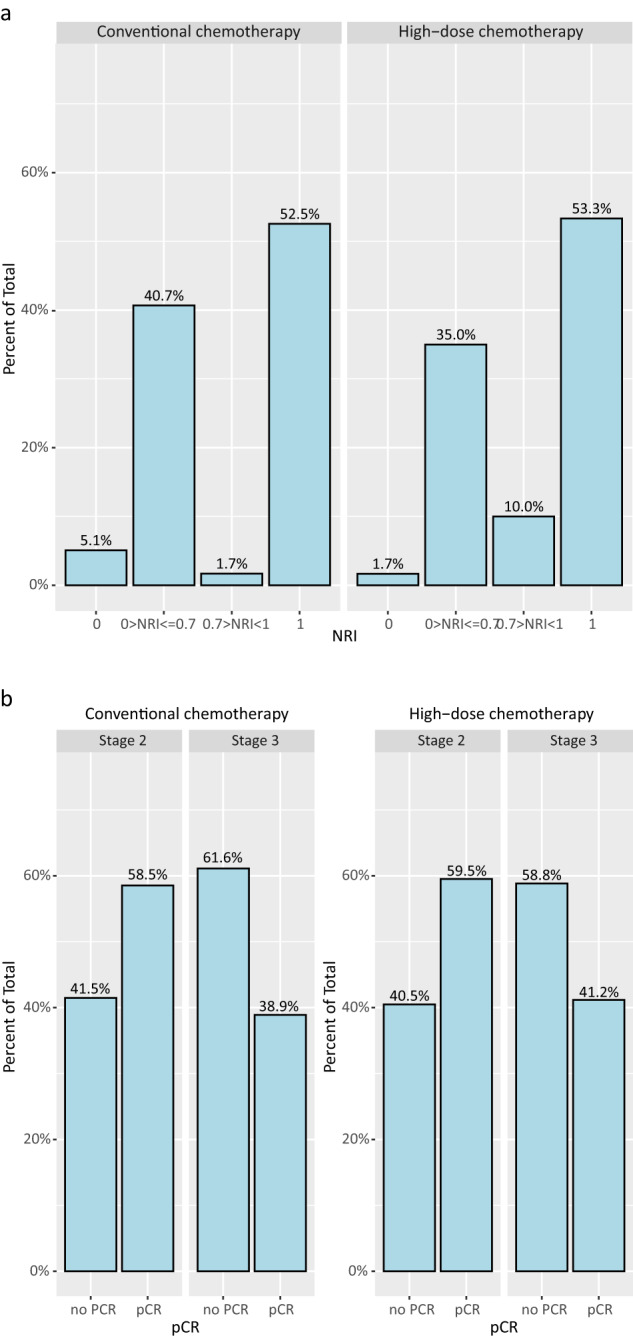
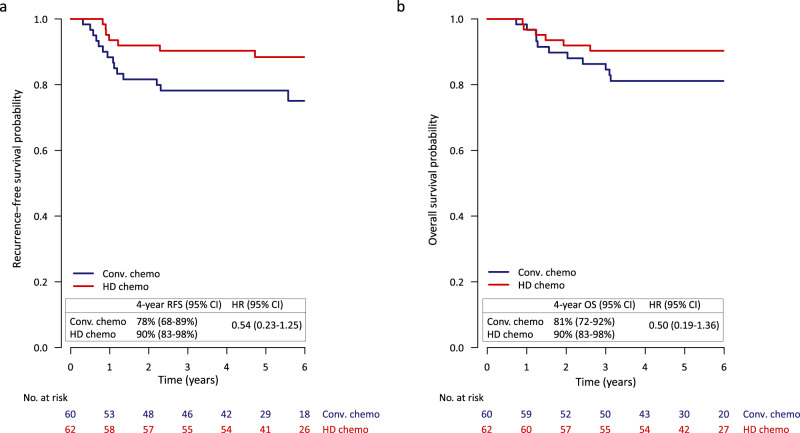
Exploratory analyses of high-dose alkylating chemotherapy trials have suggested that BRCA1 or BRCA2-pathway altered (BRCA-altered) breast cancer might be particularly sensitive to this type of treatment. In this study, patients with BRCA-altered tumors who had received three initial courses of dose-dense doxorubicin and cyclophosphamide (ddAC), were randomized between a fourth ddAC course followed by high-dose carboplatin-thiotepa-cyclophosphamide or conventional chemotherapy (initially ddAC only or ddAC-capecitabine/decetaxel [CD] depending on MRI response, after amendment ddAC-carboplatin/paclitaxel [CP] for everyone). The primary endpoint was the neoadjuvant response index (NRI). Secondary endpoints included recurrence-free survival (RFS) and overall survival (OS). In total, 122 patients were randomized. No difference in NRI-score distribution (p = 0.41) was found. A statistically non-significant RFS difference was found (HR 0.54; 95% CI 0.23-1.25; p = 0.15). Exploratory RFS analyses showed benefit in stage III (n = 35; HR 0.16; 95% CI 0.03-0.75), but not stage II (n = 86; HR 1.00; 95% CI 0.30-3.30) patients. For stage III, 4-year RFS was 46% (95% CI 24-87%), 71% (95% CI 48-100%) and 88% (95% CI 74-100%), for ddAC/ddAC-CD, ddAC-CP and high-dose chemotherapy, respectively. No significant differences were found between high-dose and conventional chemotherapy in stage II-III, triple-negative, BRCA-altered breast cancer patients. Further research is needed to establish if there are patients with stage III, triple negative BRCA-altered breast cancer for whom outcomes can be improved with high-dose alkylating chemotherapy or whether the current standard neoadjuvant therapy including carboplatin and an immune checkpoint inhibitor is sufficient. Trial Registration: NCT01057069.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare that they have no financial or non-financial interest in the subject matter or materials discussed in this manuscript. S.C.L. does have a pending patent application for a
Figures

References
-
- Farquhar, C., Marjoribanks, J., Lethaby, A. & Azhar, M. High-dose chemotherapy and autologous bone marrow or stem cell transplantation versus conventional chemotherapy for women with early poor prognosis breast cancer. Cochrane Database Syst. Rev. CD003139, 10.1002/14651858.CD003139.pub3 (2016). - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
