

Aldosterone Synthase Inhibition With Lorundrostat for Uncontrolled Hypertension: The Target-HTN Randomized Clinical Trial
- PMID: 37690061
- PMCID: PMC10493865
- DOI: 10.1001/jama.2023.16029
Aldosterone Synthase Inhibition With Lorundrostat for Uncontrolled Hypertension: The Target-HTN Randomized Clinical Trial
Abstract
Importance: Excess aldosterone production contributes to hypertension in both classical hyperaldosteronism and obesity-associated hypertension. Therapies that reduce aldosterone synthesis may lower blood pressure.
Objective: To compare the safety and efficacy of lorundrostat, an aldosterone synthase inhibitor, with placebo, and characterize dose-dependent safety and efficacy to inform dose selection in future trials.
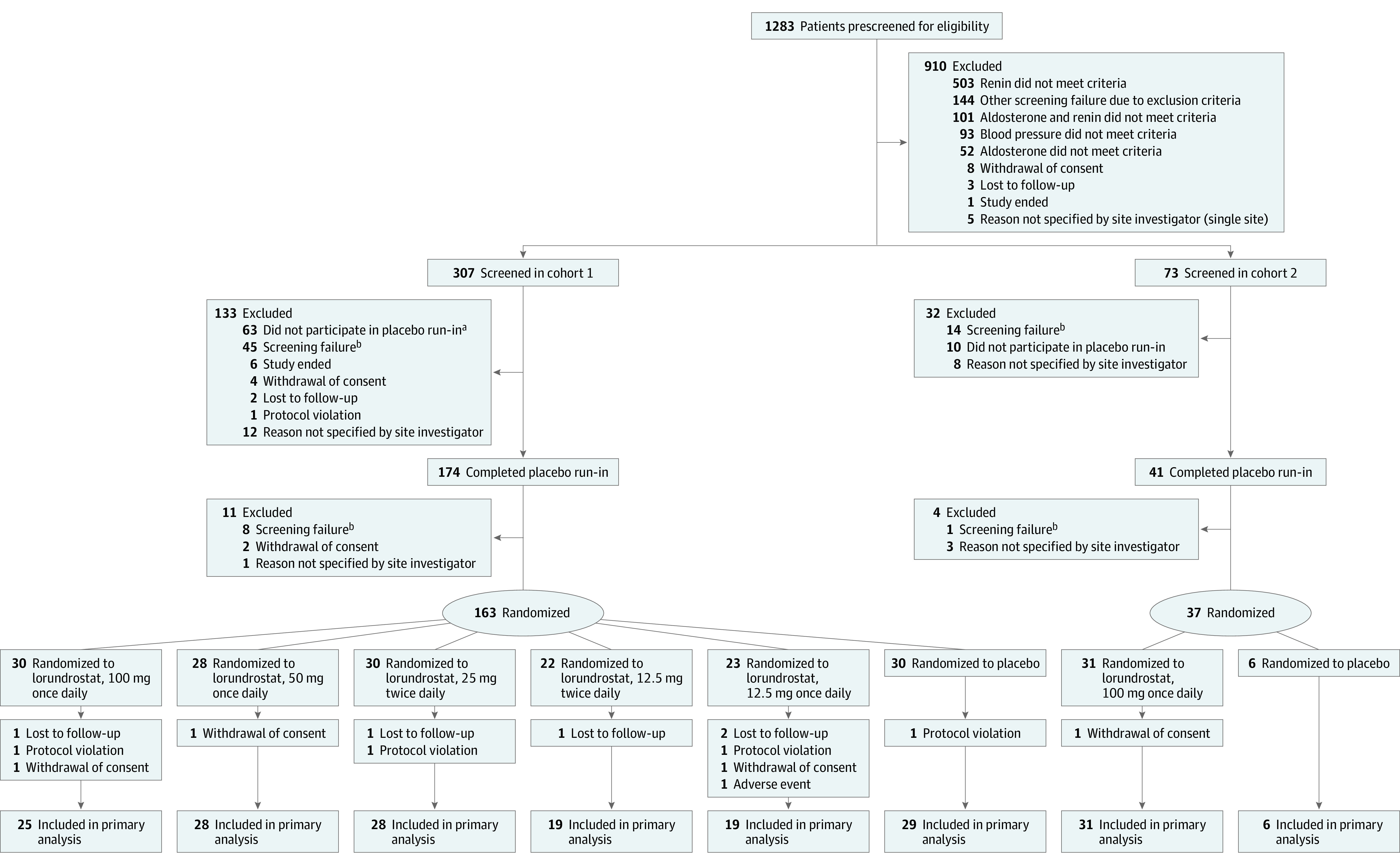
Design, setting, and participants: Randomized, placebo-controlled, dose-ranging trial among adults with uncontrolled hypertension taking 2 or more antihypertensive medications. An initial cohort of 163 participants with suppressed plasma renin (plasma renin activity [PRA] ≤1.0 ng/mL/h) and elevated plasma aldosterone (≥1.0 ng/dL) were enrolled, with subsequent enrollment of 37 participants with PRA greater than 1.0 ng/mL/h.
Interventions: Participants were randomized to placebo or 1 of 5 dosages of lorundrostat in the initial cohort (12.5 mg, 50 mg, or 100 mg once daily or 12.5 mg or 25 mg twice daily). In the second cohort, participants were randomized in a 1:6 ratio to placebo or lorundrostat, 100 mg once daily.
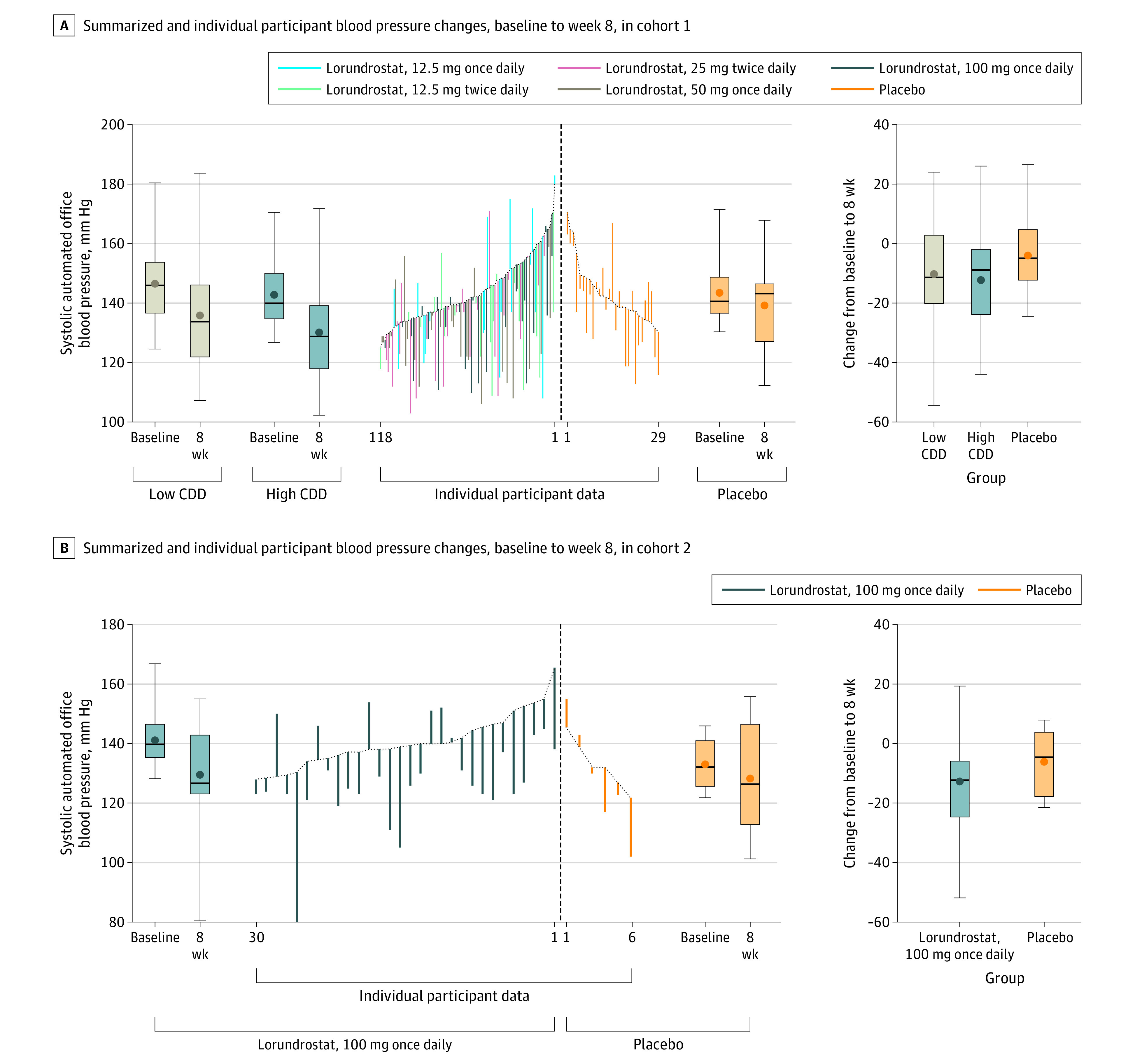
Main outcomes and measures: The primary end point was change in automated office systolic blood pressure from baseline to study week 8.
Results: Between July 2021 and June 2022, 200 participants were randomized, with final follow-up in September 2022. Following 8 weeks of treatment in participants with suppressed PRA, changes in office systolic blood pressure of -14.1, -13.2, -6.9, and -4.1 mm Hg were observed with 100 mg, 50 mg, and 12.5 mg once daily of lorundrostat and placebo, respectively. Observed reductions in systolic blood pressure in individuals receiving twice-daily doses of 25 mg and 12.5 mg of lorundrostat were -10.1 and -13.8 mm Hg, respectively. The least-squares mean difference between placebo and treatment in systolic blood pressure was -9.6 mm Hg (90% CI, -15.8 to -3.4 mm Hg; P = .01) for the 50-mg once-daily dose and -7.8 mm Hg (90% CI, -14.1 to -1.5 mm Hg; P = .04) for 100 mg daily. Among participants without suppressed PRA, 100 mg once daily of lorundrostat decreased systolic blood pressure by 11.4 mm Hg (SD, 2.5 mm Hg), which was similar to blood pressure reduction among participants with suppressed PRA receiving the same dose. Six participants had increases in serum potassium above 6.0 mmol/L that corrected with dose reduction or drug discontinuation. No instances of cortisol insufficiency occurred.
Conclusions and relevance: Among individuals with uncontrolled hypertension, use of lorundrostat was effective at lowering blood pressure compared with placebo, which will require further confirmatory studies.
Trial registration: ClinicalTrials.gov Identifier: NCT05001945.
Conflict of interest statement
Figures
Comment in
-
A New Dawn for Aldosterone as a Therapeutic Target in Hypertension.JAMA. 2023 Sep 26;330(12):1138-1139. doi: 10.1001/jama.2023.17087. JAMA. 2023. PMID: 37690088 No abstract available.
References
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023;147(8):e93-e621. doi: 10.1161/CIR.0000000000001123 - DOI - PMC - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
