

Amyloid and tau-PET in early-onset AD: Baseline data from the Longitudinal Early-onset Alzheimer's Disease Study (LEADS)
- PMID: 37690109
- PMCID: PMC10807231
- DOI: 10.1002/alz.13453
Amyloid and tau-PET in early-onset AD: Baseline data from the Longitudinal Early-onset Alzheimer's Disease Study (LEADS)
Abstract
Introduction: We aimed to describe baseline amyloid-beta (Aβ) and tau-positron emission tomograrphy (PET) from Longitudinal Early-onset Alzheimer's Disease Study (LEADS), a prospective multi-site observational study of sporadic early-onset Alzheimer's disease (EOAD).
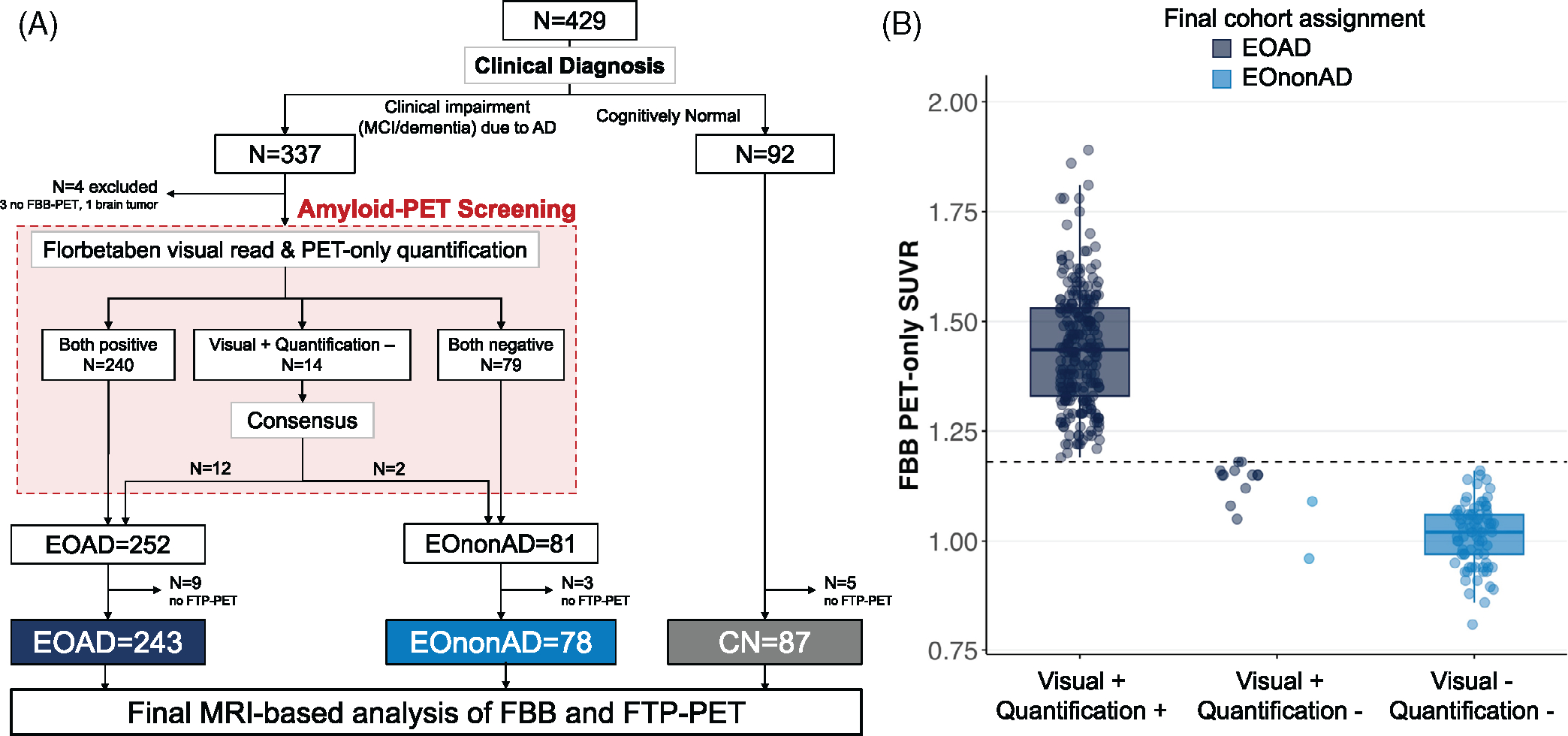
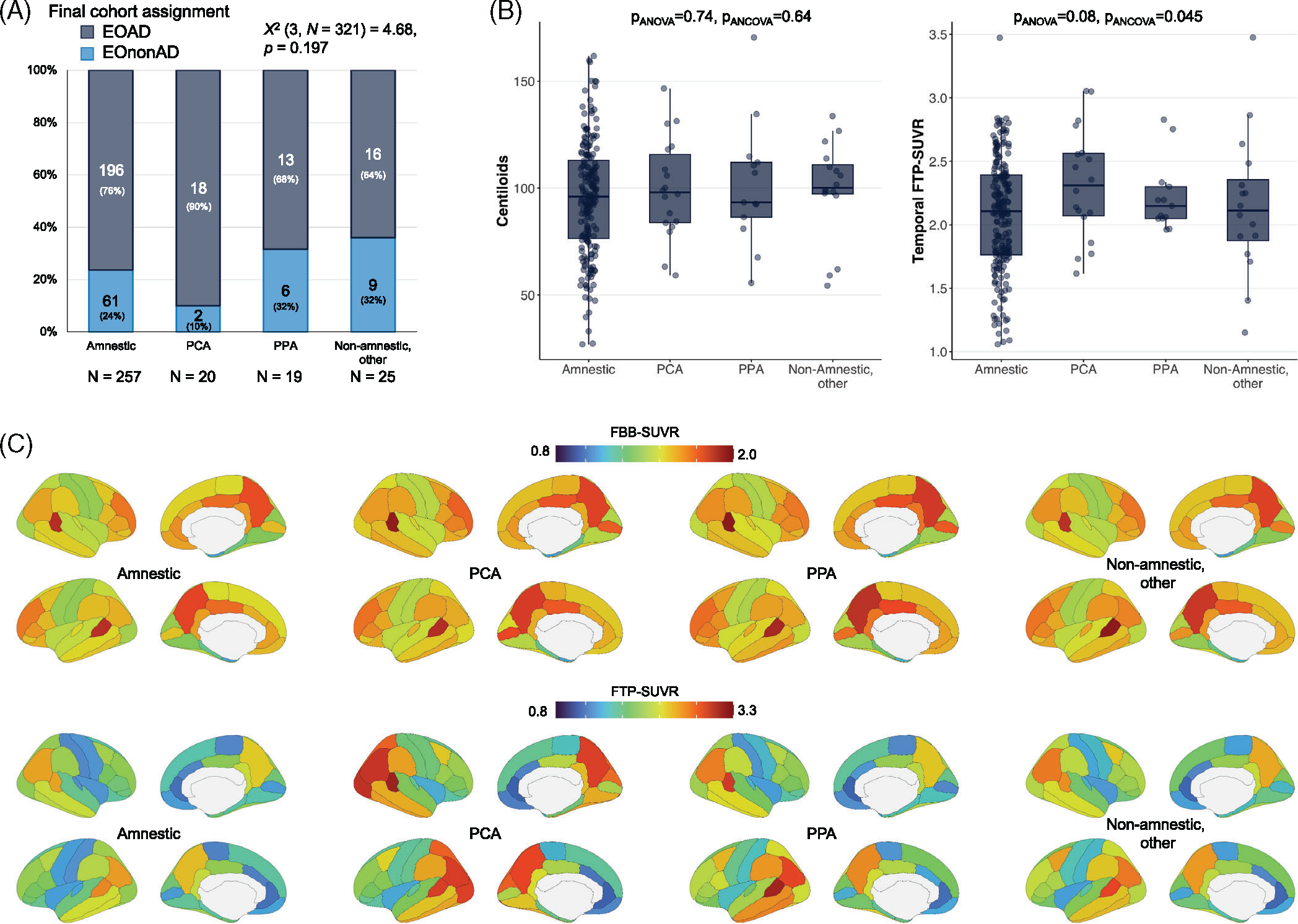
Methods: We analyzed baseline [18F]Florbetaben (Aβ) and [18F]Flortaucipir (tau)-PET from cognitively impaired participants with a clinical diagnosis of mild cognitive impairment (MCI) or AD dementia aged < 65 years. Florbetaben scans were used to distinguish cognitively impaired participants with EOAD (Aβ+) from EOnonAD (Aβ-) based on the combination of visual read by expert reader and image quantification.
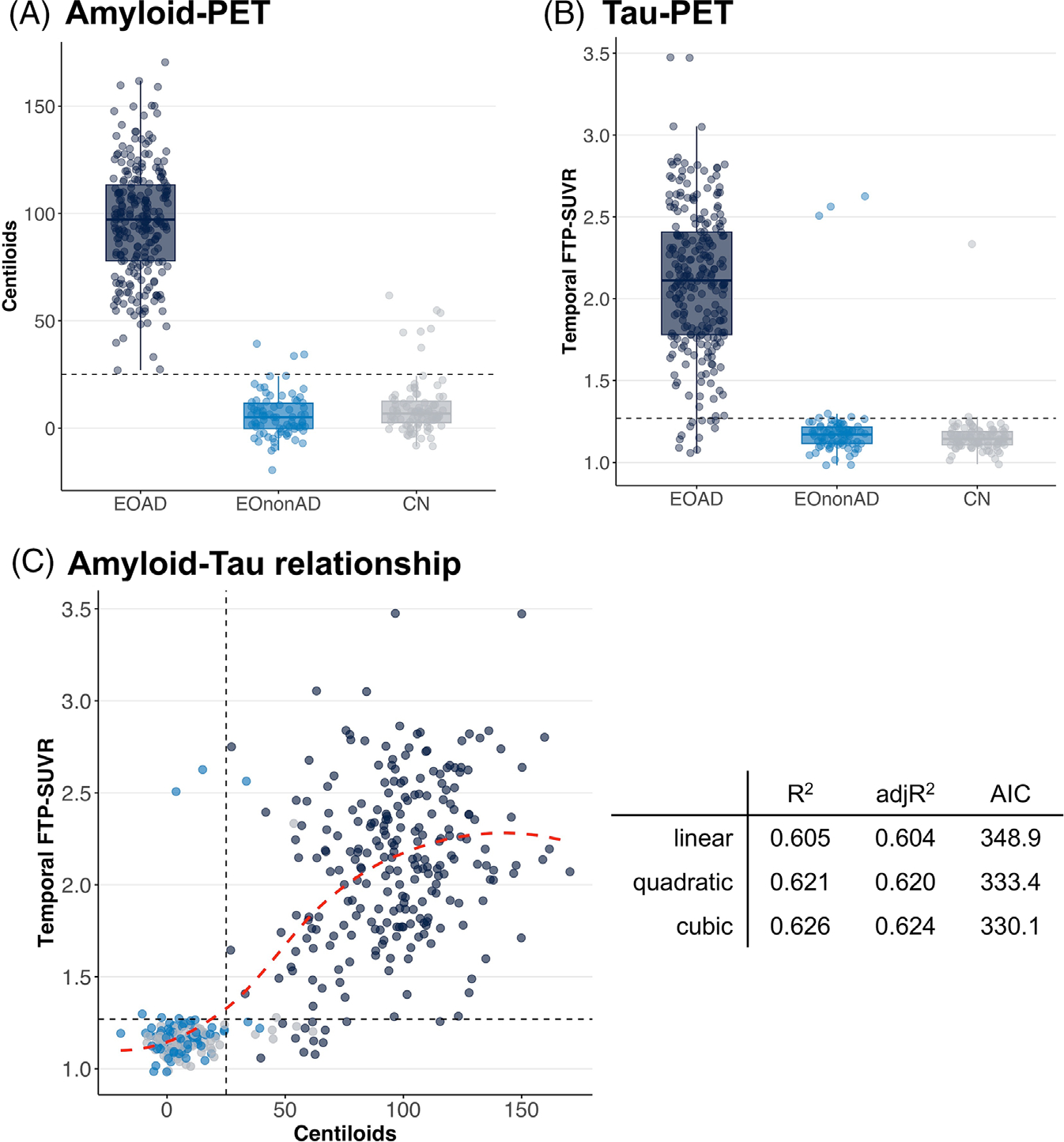
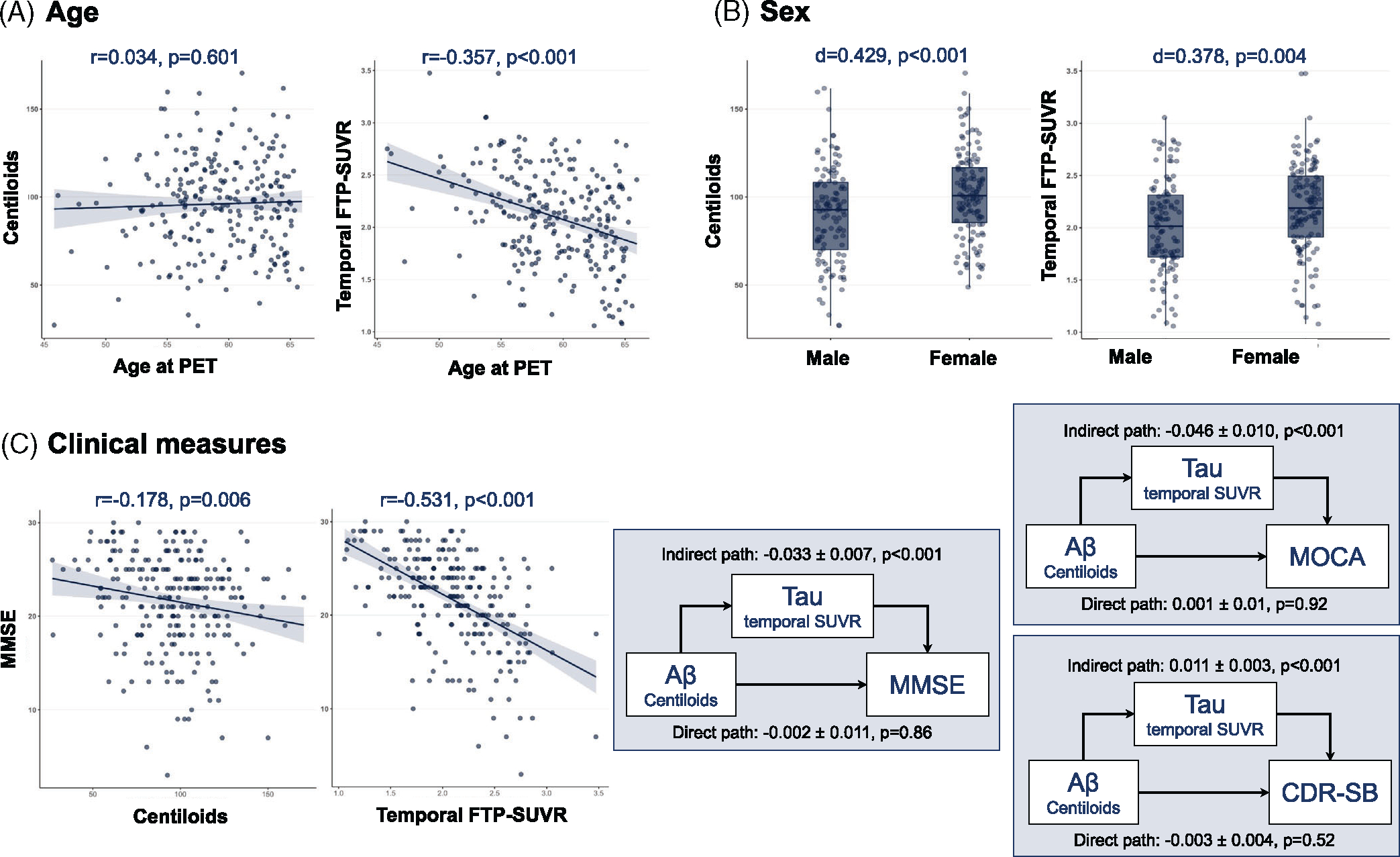
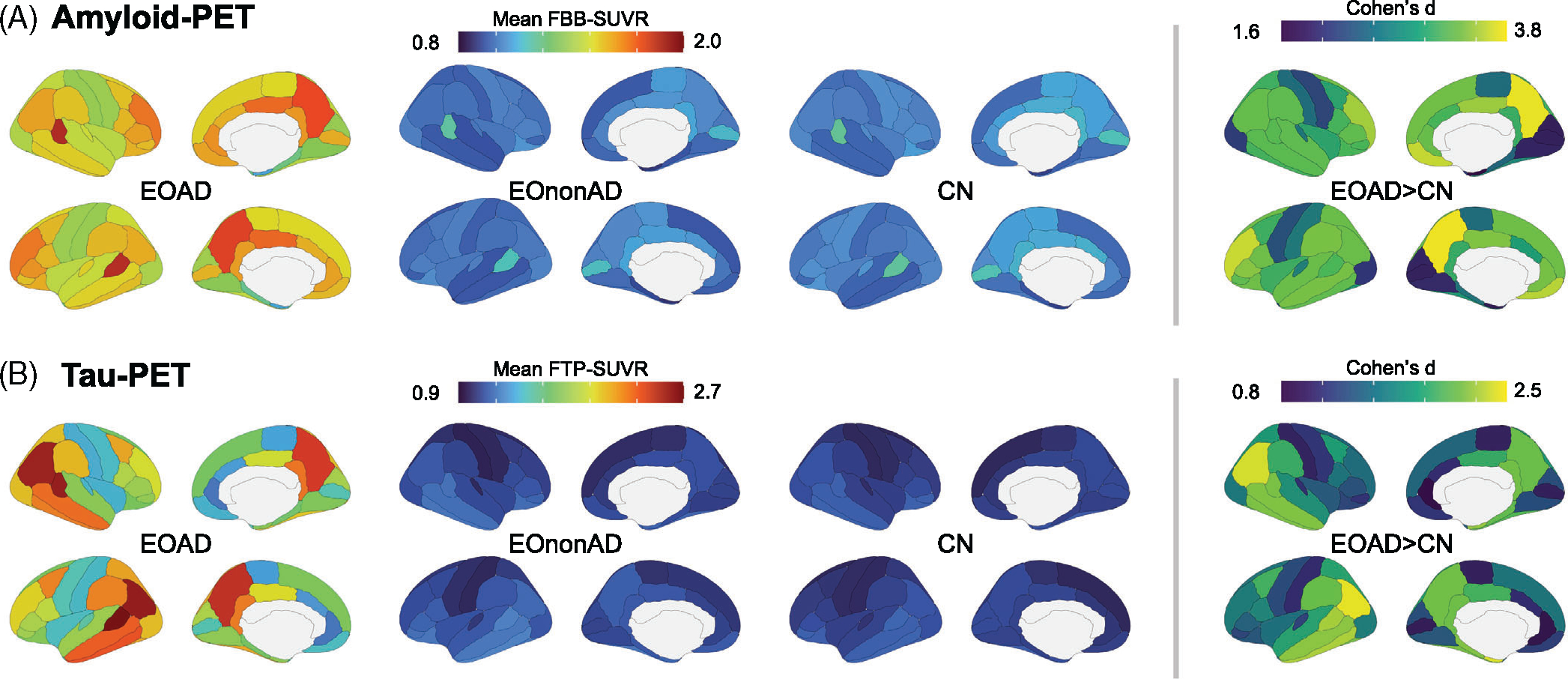
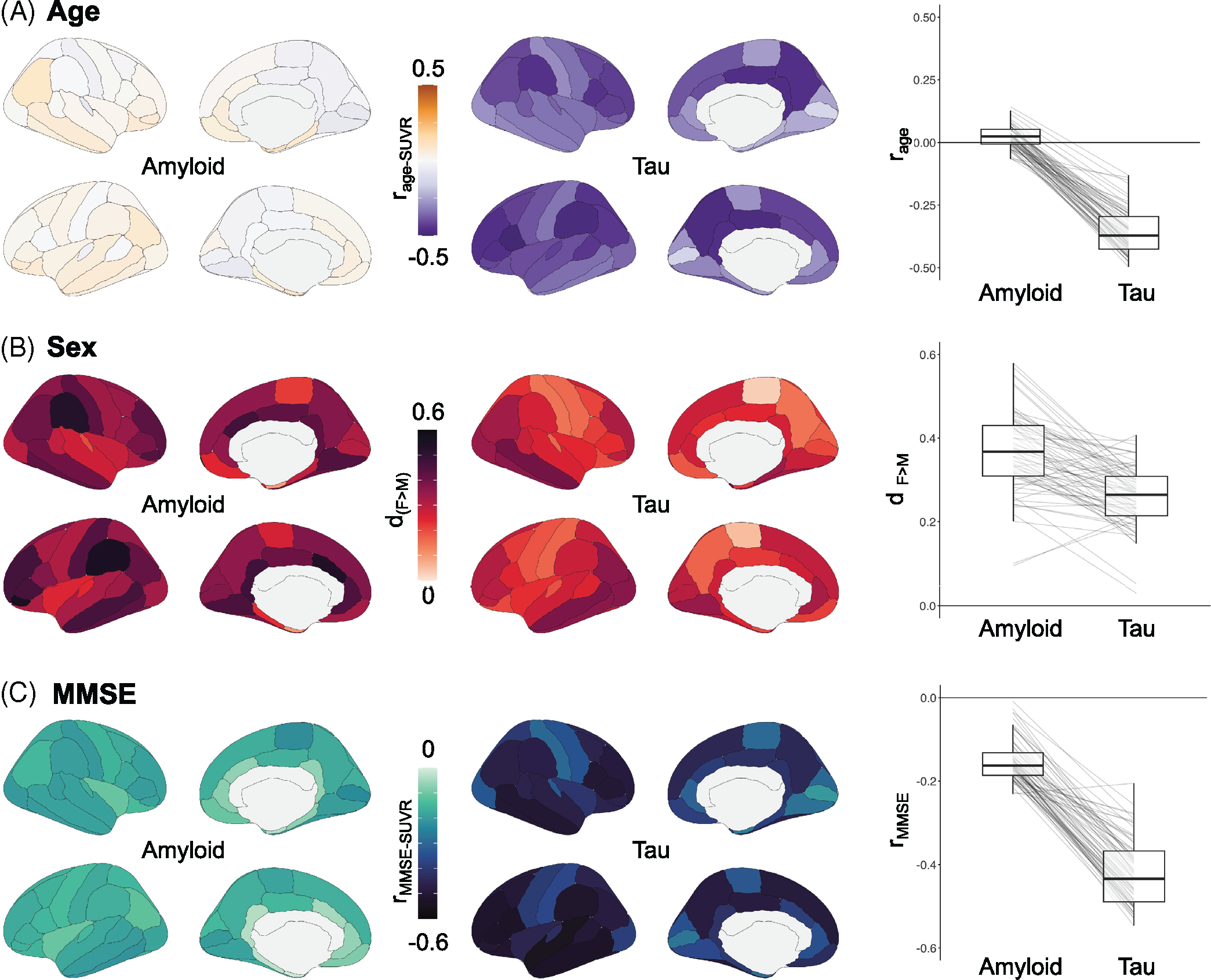
Results: 243/321 (75.7%) of participants were assigned to the EOAD group based on amyloid-PET; 231 (95.1%) of them were tau-PET positive (A+T+). Tau-PET signal was elevated across cortical regions with a parietal-predominant pattern, and higher burden was observed in younger and female EOAD participants.
Discussion: LEADS data emphasizes the importance of biomarkers to enhance diagnostic accuracy in EOAD. The advanced tau-PET binding at baseline might have implications for therapeutic strategies in patients with EOAD.
Highlights: 72% of patients with clinical EOAD were positive on both amyloid- and tau-PET. Amyloid-positive patients with EOAD had high tau-PET signal across cortical regions. In EOAD, tau-PET mediated the relationship between amyloid-PET and MMSE. Among EOAD patients, younger onset and female sex were associated with higher tau-PET.
Keywords: Alzheimer's disease; EOAD; LEADS; amyloid-PET; atypical AD; centiloids; early-onset; sex differences; tau-PET.
© 2023 The Authors. Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
CONFLICT OF INTEREST STATEMENT
Dr. Cho has nothing to disclose. Ms. Mundada has nothing to disclose. Dr. Apostolova served as a paid consultant for Biogen and Two Labs, serves on a DSMB for IQVIA, and receives research support from the NIH, the Alzheimer’s Association, Roche, Life Molecular Imaging, and Eli Lilly. Dr. Carrillo has nothing to disclose. Ms. Shankar has nothing to disclose. Ms. Amuiri has nothing to disclose. Dr. Zeltzer has nothing to disclose. Dr. Windon has nothing to disclose. Dr. Soleimani-Meigooni has nothing to disclose. Dr. Tanner has nothing to disclose. Dr. Lawhn Heath has nothing to disclose. Dr. Lesman-Segev has nothing to disclose. Dr. Aisen reports grants from NIA, FNIH, the Alzheimer’s Association, Janssen, Lilly, and Eisai, and personal fees from Merck, Roche, Biogen, Lundbeck, ImmunoBrain Checkpoint, and Samus. Dr. Eloyan has nothing to disclose. Dr. Lee has nothing to disclose. Dr. Hammers has nothing to disclose. Ms. Kirby has nothing to disclose. Dr. Dage has nothing to disclose. Dr. Fagan has received research support from Biogen, Fujirebio, and Roche Diagnostics. She is a member of the scientific advisory boards for Roche Diagnostics, Genentech, and AbbVie and consults for Araclon/Griffols, DiademRes, and Otsuka Pharmaceuticals. Dr. Foroud has nothing to disclose. Dr. Grinberg has nothing to disclose. Dr. Jack serves on an independent data monitoring board for Roche and has consulted for and served as a speaker for Eisai, but he receives no personal compensation from any commercial entity. He receives research support from the NIH and the Alexander Family Alzheimer’s Disease Research Professorship of the Mayo Clinic. Dr. Kramer has nothing to disclose. Dr. Kukull is supported by the NIA. Dr. Murray served as a paid consultant for AVID Radiopharmaceuticals and receives research support from the NIH, the Alzheimer’s Association, and the state of Florida. Dr. Nudelman has nothing to disclose. Dr. Toga has nothing to disclose. Dr. Vemuri has nothing to disclose. Dr. Atri has nothing to disclose. Dr. Day is supported by the NIA; he serves as a topic editor on dementia for DynaMed Plus (EBSCO Industries, Inc), is the clinical director for the Anti-NMDA Receptor Encephalitis Foundation and holds stocks in ANI Pharmaceuticals. Dr. Duara has nothing to disclose. Dr. Graff-Radford receives research support from Lilly, AbbVie, and Biogen. Dr. Honig has nothing to disclose. Dr. Jones has nothing to disclose. Dr. Masdeu served on the speaker’s bureau and consulted for Biogen. He received research support from the NIH, Avanir, Abbvie, Biogen, Eli Lilly, Esai, and Novartis. Dr. Mendez receives grant support from NIA and has received support from Biogen. Dr. Musiek received research funding from Eisai Pharmaceuticals Inc. Dr. Onyike has nothing to disclose. Dr. Rogalski has nothing to disclose. Dr. Salloway received consultation fees and research support from Biogen, Eisai, Lilly, Genentech, and Roche. Dr. Sha has nothing to disclose. Dr. Turner has nothing to disclose. Dr. Wingo has nothing to disclose. Dr. Wolk received grants from Eli Lilly/Avid Radiopharmaceuticals, Merck, and Biogen, and consulted for Merck, Janssen, and GE Healthcare. Dr. Koeppe has nothing to disclose. Dr. Iaccarino is currently a full-time employee of Eli Lilly and Company / Avid Radiopharmaceuticals and a minor shareholder of Eli Lilly and Company. His contribution to the work presented in this manuscript was performed while he was affiliated with the University of California San Francisco. Dr. Dickerson receives research support from the NIH and the Alzheimer’s Drug Discovery Foundation. He consulted for Arkuda, Axovant, Lilly, Biogen, Merck, Novartis, and Wave LifeSciences. He is editor for Neuroimage: Clinical and Cortex. He receives royalties from Oxford University Press and Cambridge University Press. Dr. La Joie is an Associate Editor for Alzheimer’s Research & Therapy. Dr. Rabinovici receives research funding from Avid Radiopharmaceuticals, GE Healthcare, Life Molecular Imaging, Genentech. He has received consulting fees from Alector, Eli Lilly, Genentech, Roche, Merck. He receives fees for serving on a DSMB for Johnson & Johnson. He is an Associate Editor for JAMA Neurology The authors have no conflicts of interest to declare supporting information.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- U19 NS110456/NS/NINDS NIH HHS/United States
- R56 AG057195/AG/NIA NIH HHS/United States
- U24 AG021886/AG/NIA NIH HHS/United States
- U01 AG057195/AG/NIA NIH HHS/United States
- R01 AG072120/AG/NIA NIH HHS/United States
- P30 AG072980/AG/NIA NIH HHS/United States
- R21 NS120629/NS/NINDS NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- P30 AG066530/AG/NIA NIH HHS/United States
- R35 AG072362/AG/NIA NIH HHS/United States
- P30 AG066546/AG/NIA NIH HHS/United States
- P30 AG072977/AG/NIA NIH HHS/United States
- R01 AG075827/AG/NIA NIH HHS/United States
- R01 AG079170/AG/NIA NIH HHS/United States
- ZEN-21-848216/ALZ/Alzheimer's Association/United States
- P30 AG072979/AG/NIA NIH HHS/United States
