

Endogenous Glucose Production in Patients With Glycogen Storage Disease Type Ia Estimated by Oral D-[6,6-2H2]-glucose
- PMID: 37690115
- PMCID: PMC10795891
- DOI: 10.1210/clinem/dgad537
Endogenous Glucose Production in Patients With Glycogen Storage Disease Type Ia Estimated by Oral D-[6,6-2H2]-glucose
Abstract
Context: Glycogen storage disease type Ia (GSDIa) is an inborn metabolic disorder characterized by impaired endogenous glucose production (EGP). Monitoring of patients with GSDIa is prioritized because of ongoing treatment developments. Stable isotope tracers may enable reliable EGP monitoring.
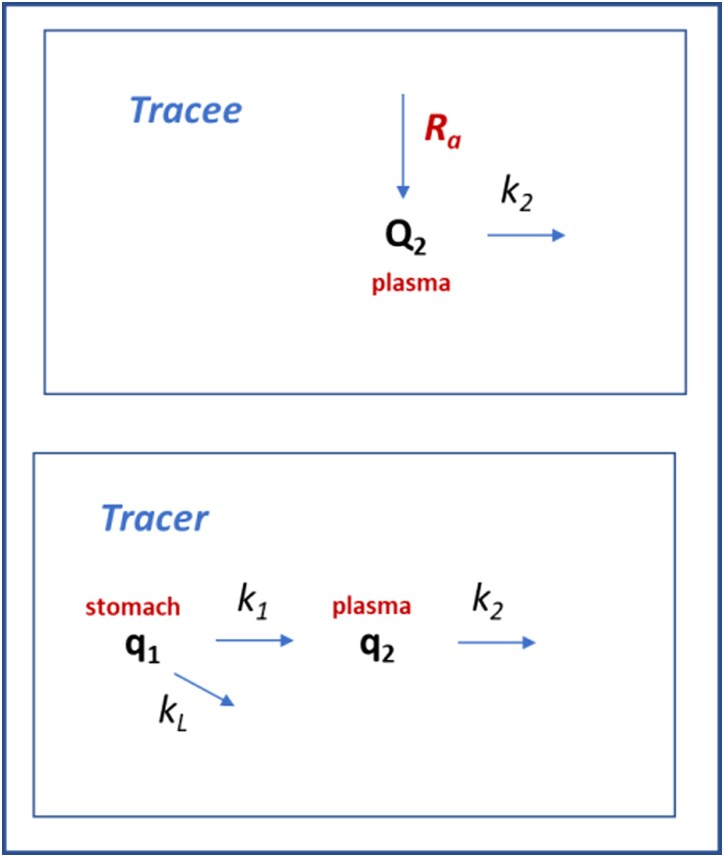
Objective: The aim of this study was to prospectively assess the rate of appearance of endogenous glucose into the bloodstream (Ra) in patients with GSDIa after a single oral D-[6,6-2H2]-glucose dose.
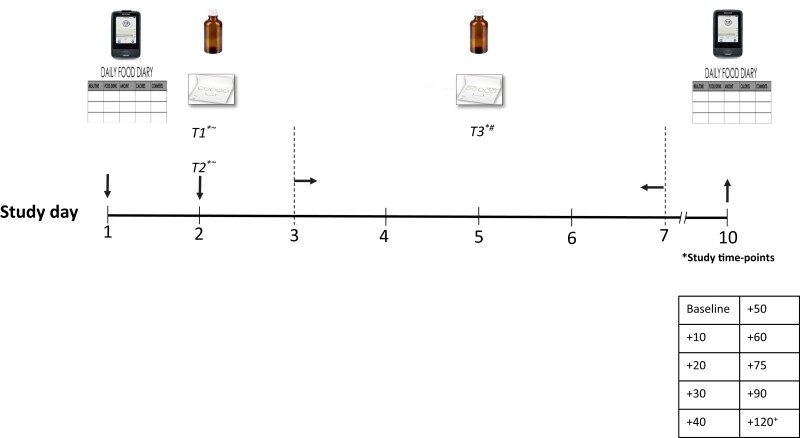
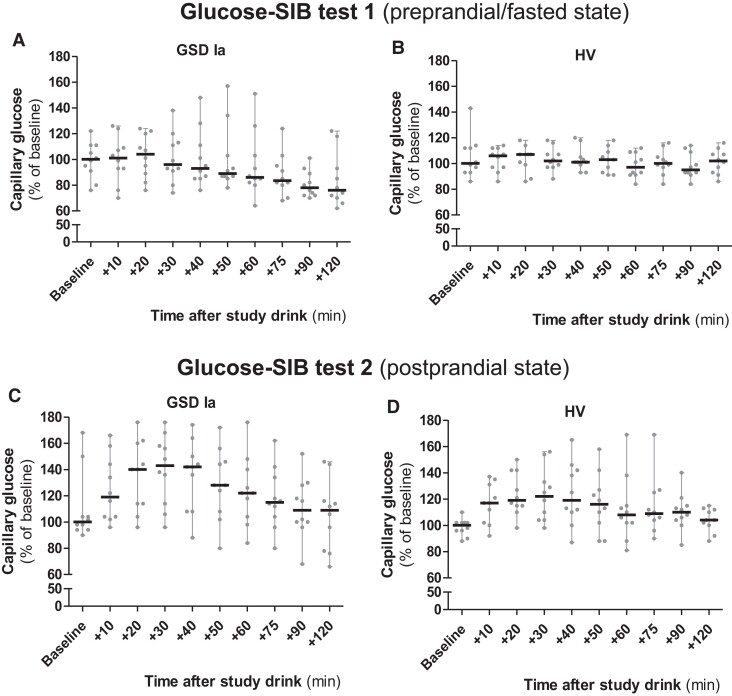
Methods: Ten adult patients with GSDIa and 10 age-, sex-, and body mass index-matched healthy volunteers (HVs) were enrolled. For each participant, 3 oral glucose tracer tests were performed: (1) preprandial/fasted, (2) postprandial, and (3) randomly fed states. Dried blood spots were collected before D-[6,6-2H2]-glucose administration and 10, 20, 30, 40, 50, 60, 75, 90, and 120 minutes thereafter.
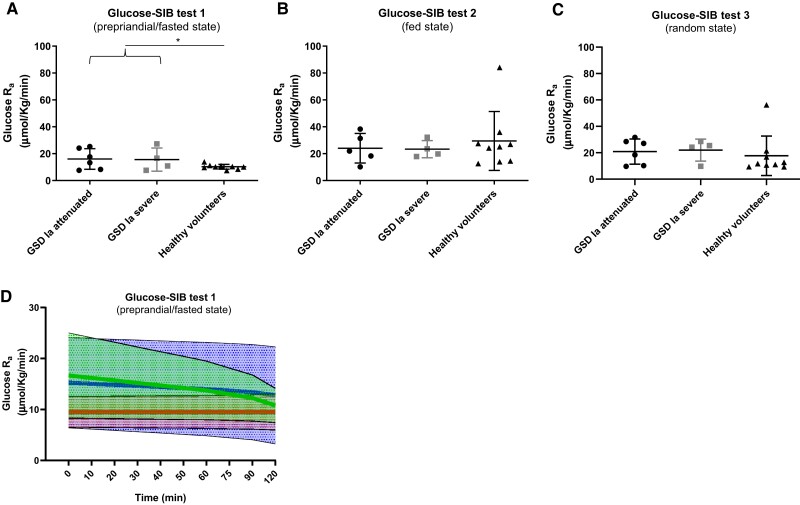
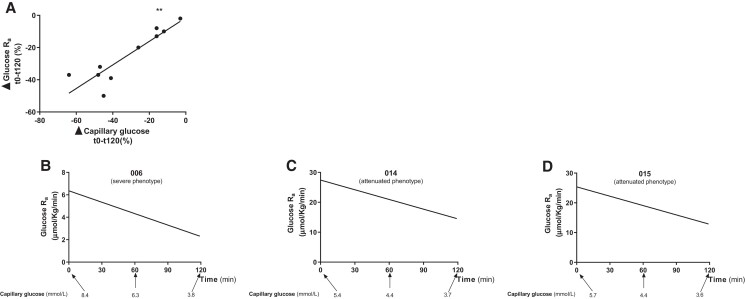
Results: Glucose Ra in fasted HVs was consistent with previously reported data. The time-averaged glucose Ra was significantly higher in (1) preprandial/fasted patients with GSDIa than HV and (2) postprandial HV compared with fasted HV(P < .05). A progressive decrease in glucose Ra was observed in preprandial/fasted patients with GSDIa; the change in glucose Ra time-course was directly correlated with the change in capillary glucose (P < .05).
Conclusion: This is the first study to quantify glucose Ra in patients with GSDIa using oral D-[6,6-2H2] glucose. The test can reliably estimate EGP under conditions in which fasting tolerance is unaffected but does not discriminate between relative contributions of EGP (eg, liver, kidney) and exogenous sources (eg, dietary cornstarch). Future application is warranted for longitudinal monitoring after novel genome based treatments in patients with GSDIa in whom nocturnal dietary management can be discontinued.
Keywords: diet; glycogen storage disease type Ia; monitoring; precision medicine; stable isotopes.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Rake JP, Visser G, Labrune P, Leonard JV, Ullrich K, Smit GP. Glycogen storage disease type I: diagnosis, management, clinical course and outcome. Results of the European study on glycogen storage disease type I (ESGSD I). Eur J Pediatr. 2002;161(1):S20‐S34. - PubMed
-
- Kishnani PS, Austin SL, Abdenur JE, et al. Diagnosis and management of glycogen storage disease type I: a practice guideline of the American college of medical genetics and genomics. Genet Med. 2014;16(11):e1. - PubMed
-
- Walter JH, Labrune P, Laforêt P. The glycogen storage diseases and related disorders. In: Saudubray JM, Baumgartner MR, García-Cazorla Á, Walter J, eds. Inborn Metabolic Diseases. Springer; 2022:179-200.
