

Platelet-derived biomaterial with hyaluronic acid alleviates temporal-mandibular joint osteoarthritis: clinical trial from dish to human
- PMID: 37691117
- PMCID: PMC10494357
- DOI: 10.1186/s12929-023-00962-y
Platelet-derived biomaterial with hyaluronic acid alleviates temporal-mandibular joint osteoarthritis: clinical trial from dish to human
Abstract
Background: Bioactive materials have now raised considerable attention for the treatment of osteoarthritis (OA), such as knee OA, rheumatoid OA, and temporomandibular joint (TMJ) OA. TMJ-OA is a common disease associated with an imbalance of cartilage regeneration, tissue inflammation, and disability in mouth movement. Recently, biological materials or molecules have been developed for TMJ-OA therapy; however, ideal treatment is still lacking. In this study, we used the combination of a human platelet rich plasma with hyaluronic acid (hPRP/HA) for TMJ-OA therapy to perform a clinical trial in dish to humans.
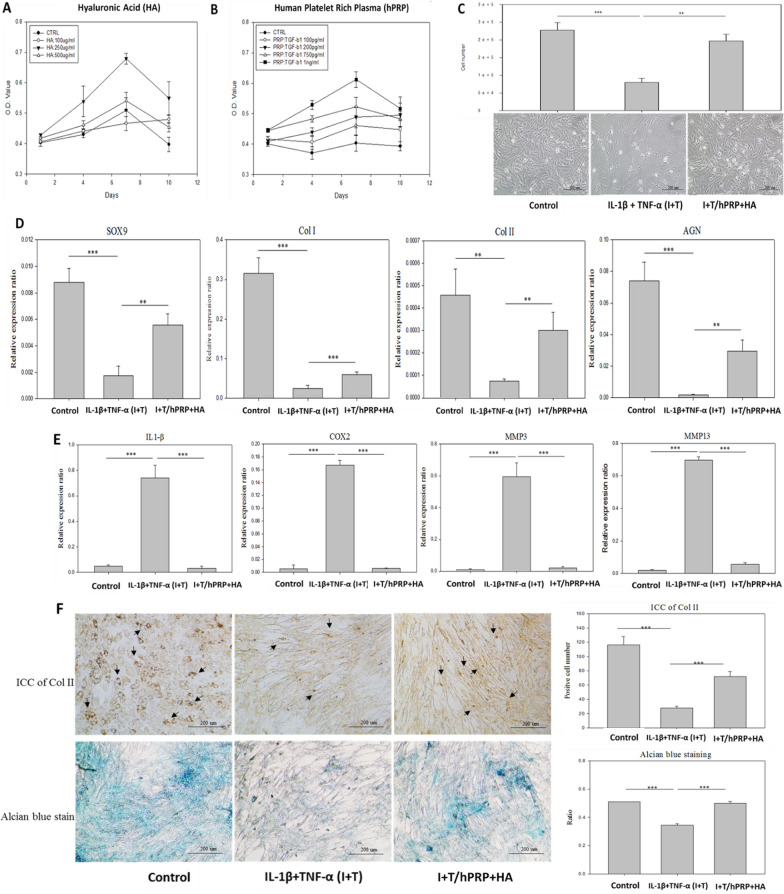
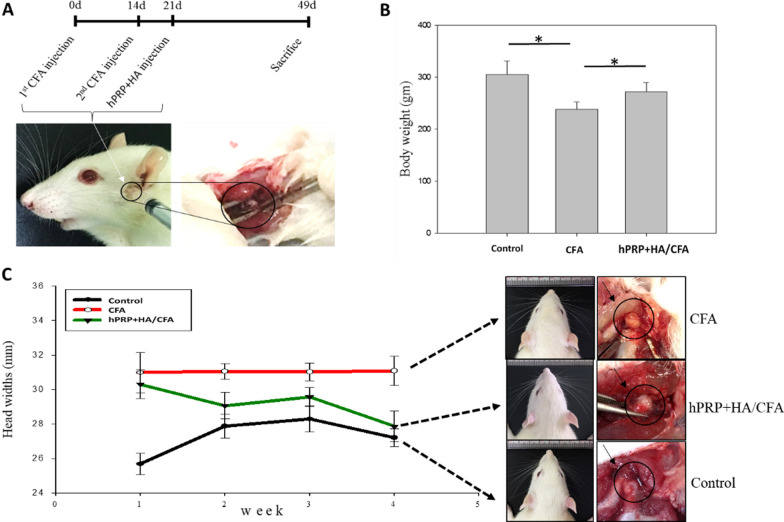
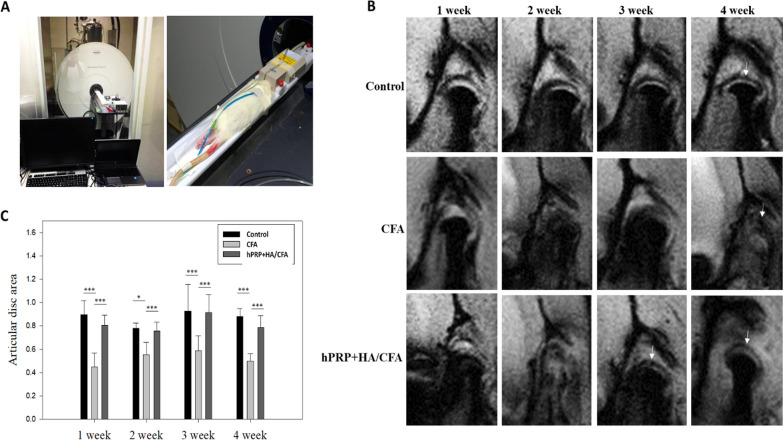
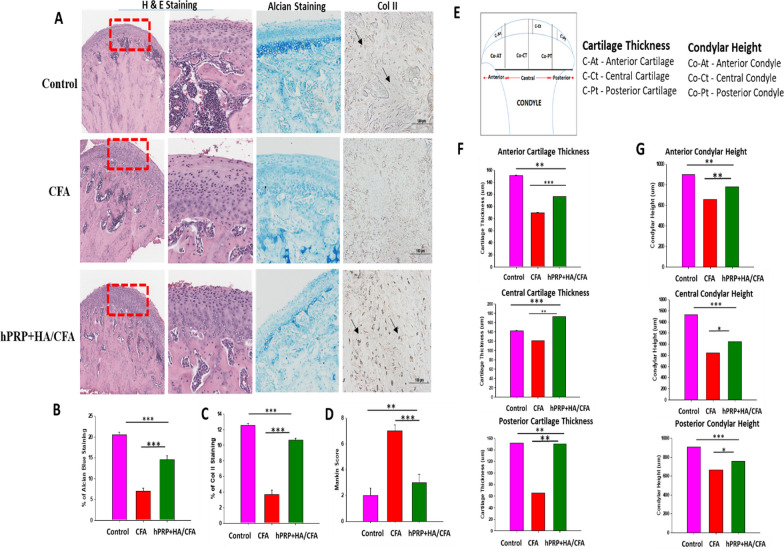
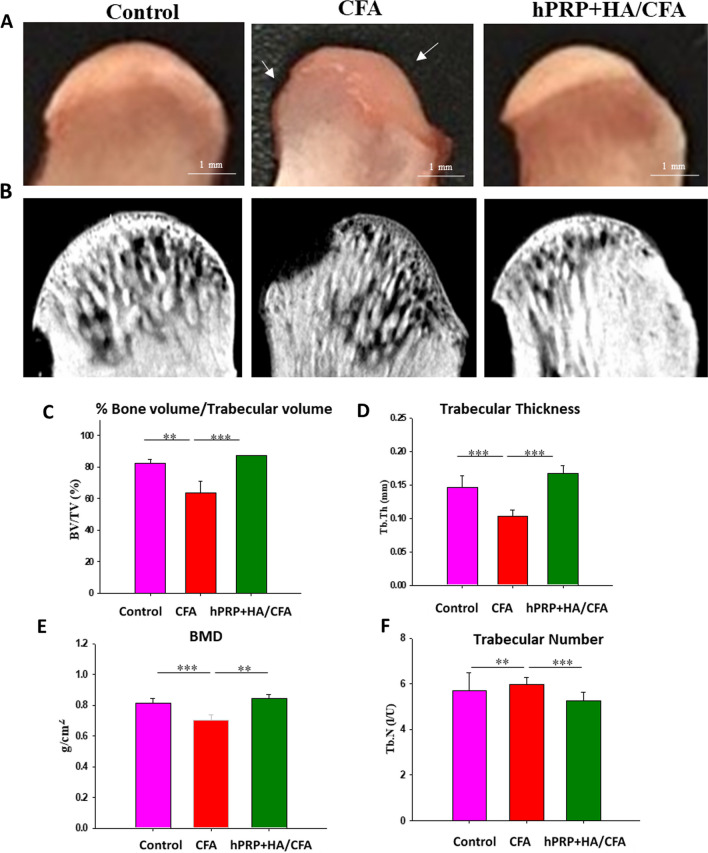
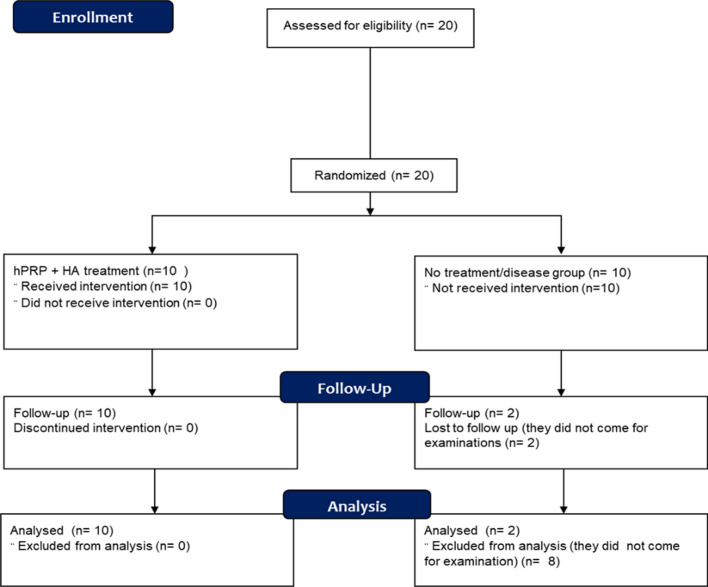
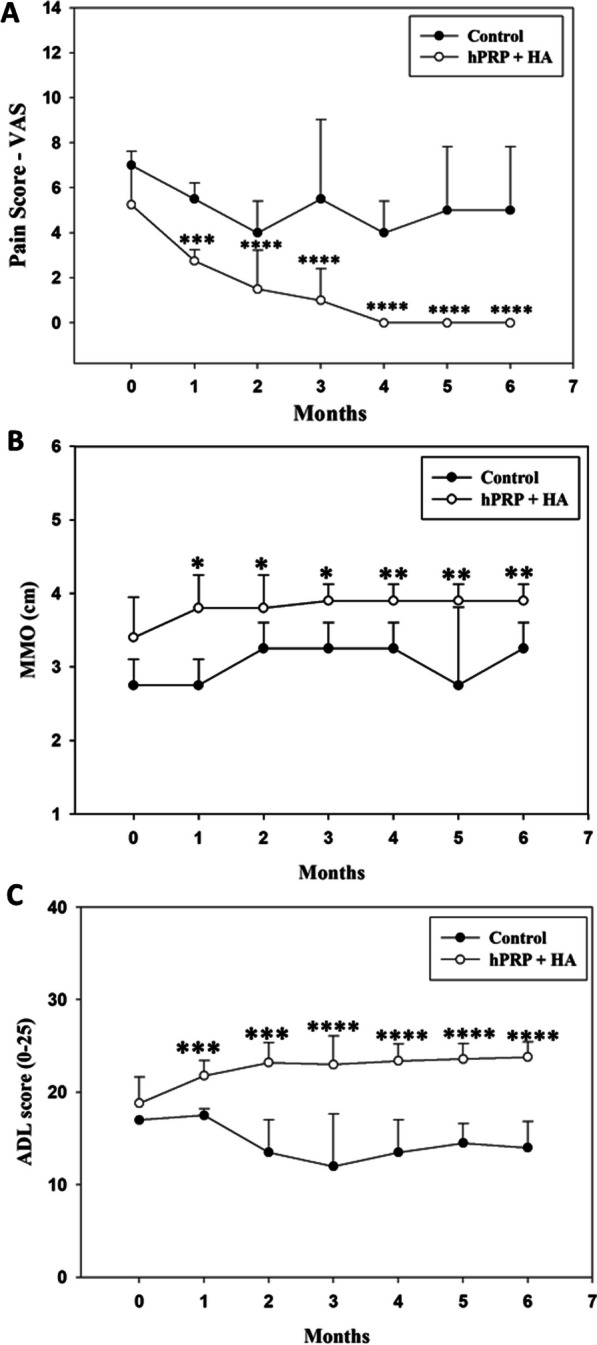
Method: Herein, hPRP was prepared, and the hPRP/HA combined concentration was optimized by MTT assay. For the clinical trial in dish, pro-inflammatory-induced in-vitro and in-vivo mimic 3D TMJ-OA models were created, and proliferation, gene expression, alcian blue staining, and IHC were used to evaluate chondrocyte regeneration. For the animal studies, complete Freund's adjuvant (CFA) was used to induce the TMJ-OA rat model, and condyle and disc regeneration were investigated through MRI. For the clinical trial in humans, 12 patients with TMJ-OA who had disc displacement and pain were enrolled. The disc displacement and pain at baseline and six months were measured by MRI, and clinical assessment, respectively.
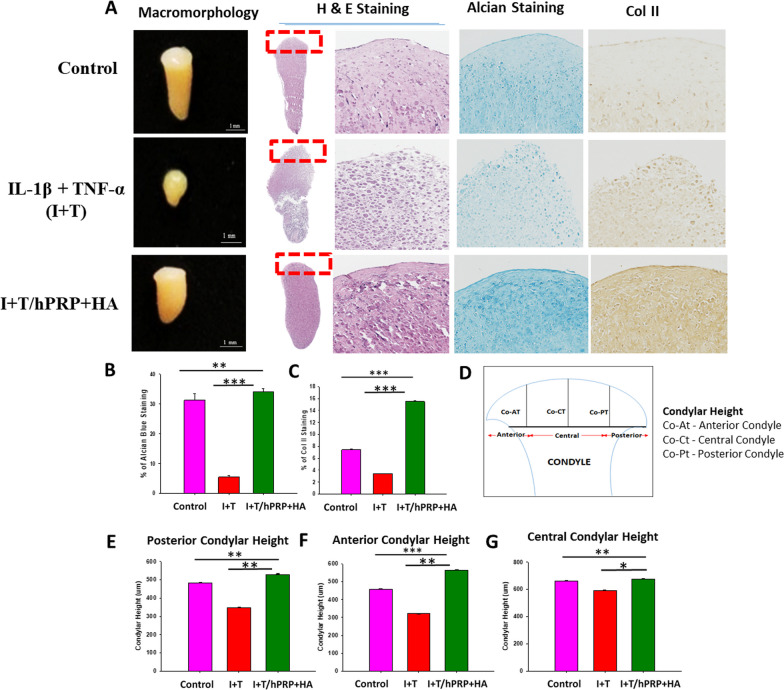
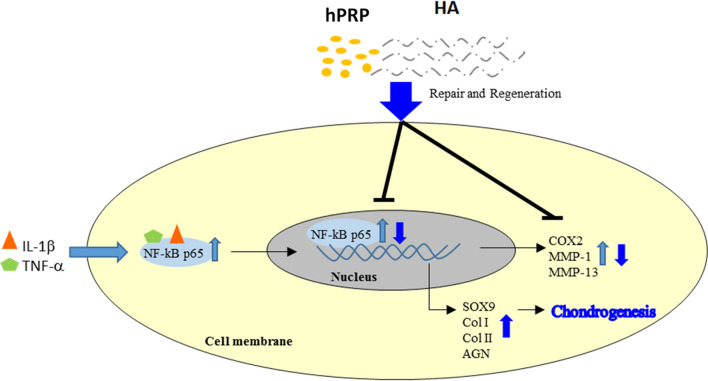
Results: Combined hPRP/HA treatment ameliorated the proinflammatory-induced TMJ-OA model and promoted chondrocyte proliferation by activating SOX9, collagen type I/II, and aggrecan. TMJ-OA pathology-related inflammatory factors were efficiently downregulated with hPRP/HA treatment. Moreover, condylar cartilage was regenerated by hPRP/HA treatment in a proinflammatory-induced 3D neocartilage TMJ-OA-like model. During the animal studies, hPRP/HA treatment strongly repaired the condyle and disc in a CFA-induced TMJ-OA rat model. Furthermore, we performed a clinical trial in humans, and the MRI data demonstrated that after 6 months of treatment, hPRP/HA regenerated the condylar cartilage, reduced disc displacement, alleviated pain, and increased the maximum mouth opening (MMO). Overall, clinical trials in dish to human results revealed that hPRP/HA promoted cartilage regeneration, inhibited inflammation, reduced pain, and increased joint function in TMJ-OA.
Conclusion: Conclusively, this study highlighted the therapeutic potential of the hPRP and HA combination for TMJ-OA therapy, with detailed evidence from bench to bedside. Trial registration Taipei Medical University Hospital (TMU-JIRB No. N201711041). Registered 24 November 2017. https://tmujcrc.tmu.edu.tw/inquiry_general.php .
Keywords: Clinical trial; Hyaluronic acid; Platelet-derived biomaterial; TMJ-OA.
© 2023. National Science Council of the Republic of China (Taiwan).
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Zhang S, Teo KYW, Chuah SJ, Lai RC, Lim SK, Toh WS. MSC exosomes alleviate temporomandibular joint osteoarthritis by attenuating inflammation and restoring matrix homeostasis. Biomaterials. 2019;200:35–47. - PubMed
-
- Wang XD, Zhang JN, Gan YH, Zhou YH. Current understanding of pathogenesis and treatment of TMJ osteoarthritis. J Dent Res. 2015;94(5):666–673. - PubMed
-
- Le ADK, Enweze L, DeBaun MR, Dragoo JL. Platelet-rich plasma. Clin Sports Med. 2019;38(1):17–44. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
