

Disease Course, Treatments, and Outcomes of Children With Systemic Juvenile Idiopathic Arthritis-Associated Lung Disease
- PMID: 37691306
- PMCID: PMC11156420
- DOI: 10.1002/acr.25234
Disease Course, Treatments, and Outcomes of Children With Systemic Juvenile Idiopathic Arthritis-Associated Lung Disease
Abstract
Objective: Systemic juvenile idiopathic arthritis-associated lung disease (SJIA-LD) is a life-threatening disease complication. Key questions remain regarding clinical course and optimal treatment approaches. The objectives of the study were to detail management strategies after SJIA-LD detection, characterize overall disease courses, and measure long-term outcomes.
Methods: This was a prospective cohort study. Clinical data were abstracted from the electronic medical record, including current clinical status and changes since diagnosis. Serum biomarkers were determined and correlated with presence of LD.
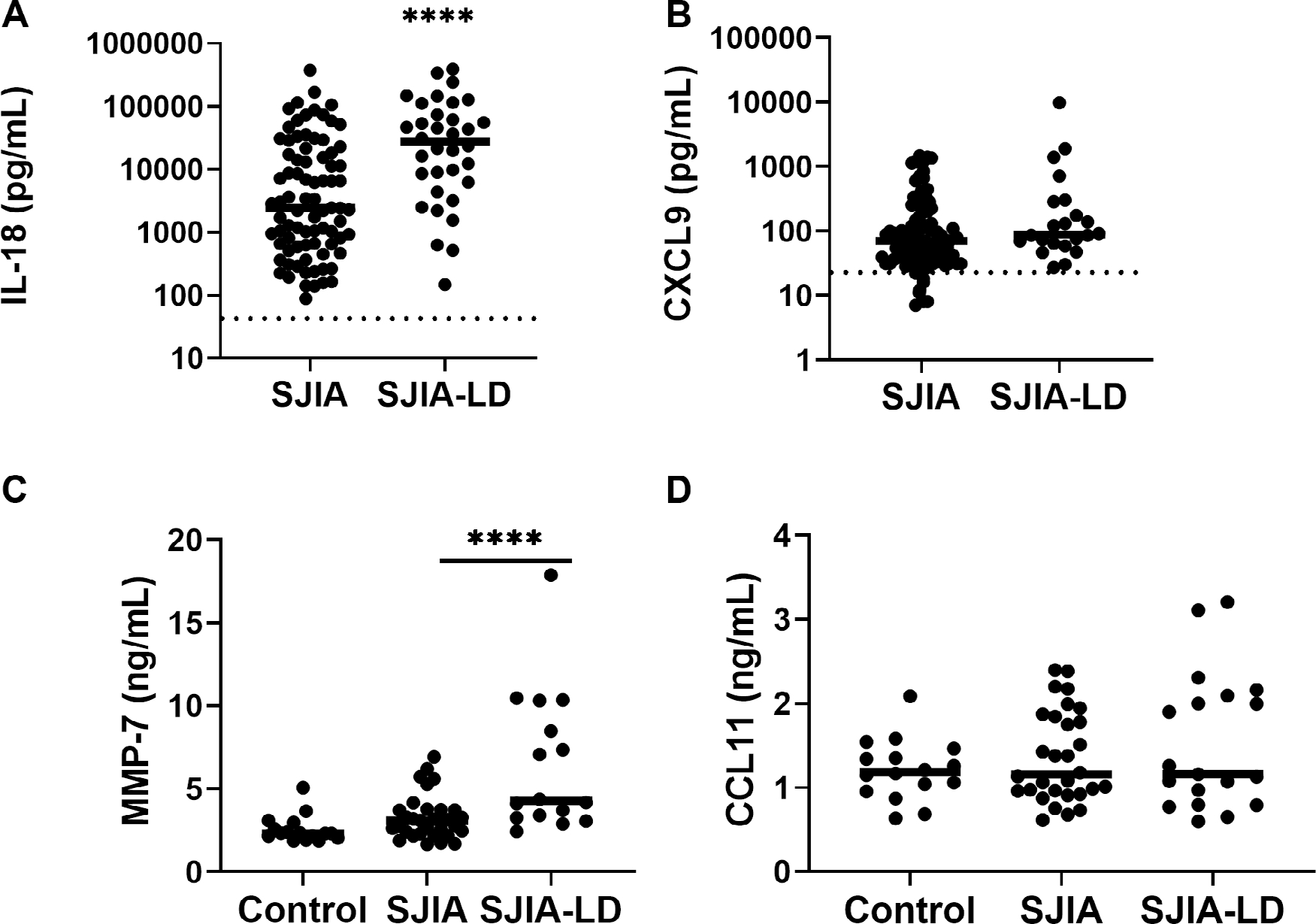
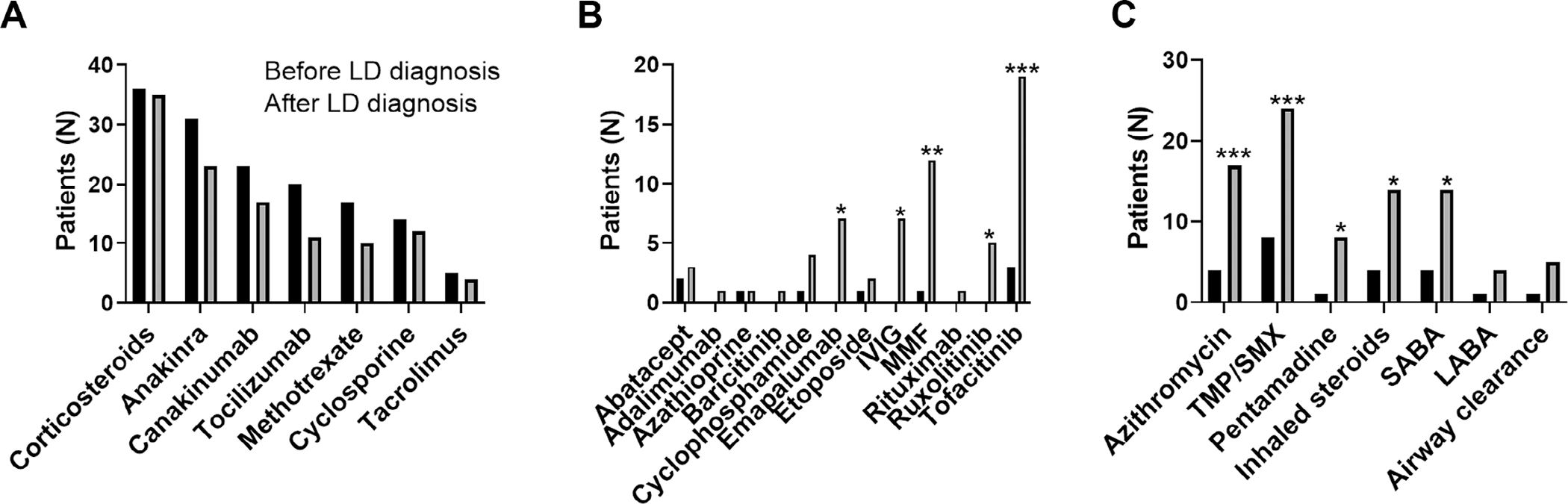
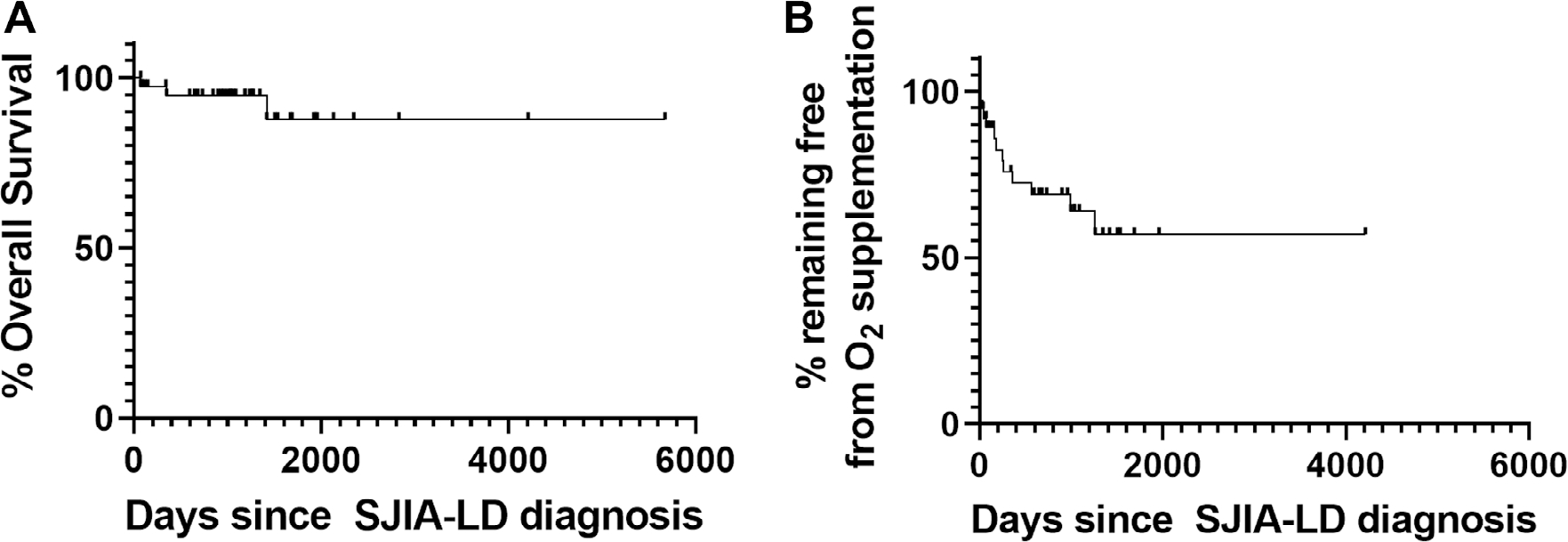
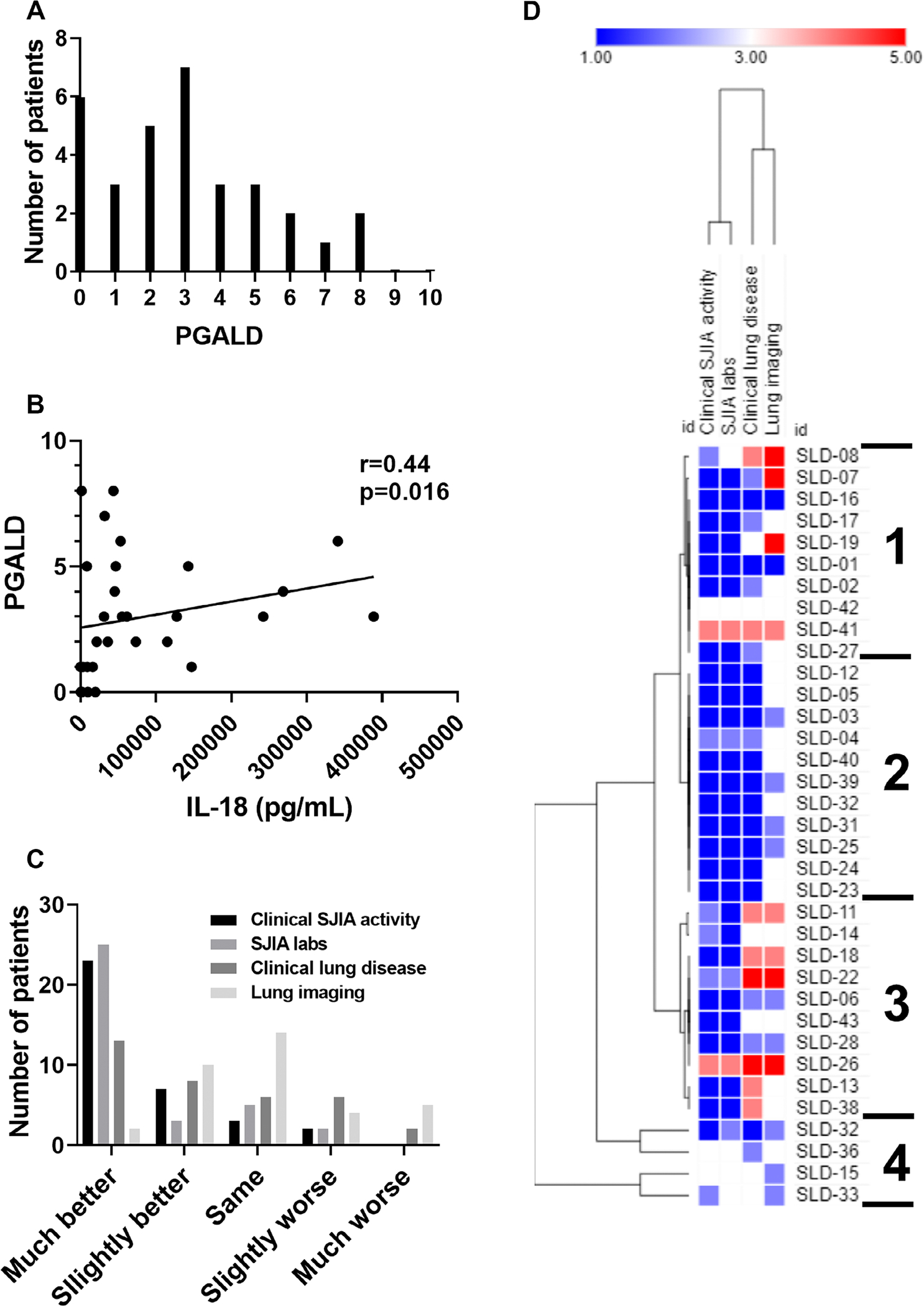
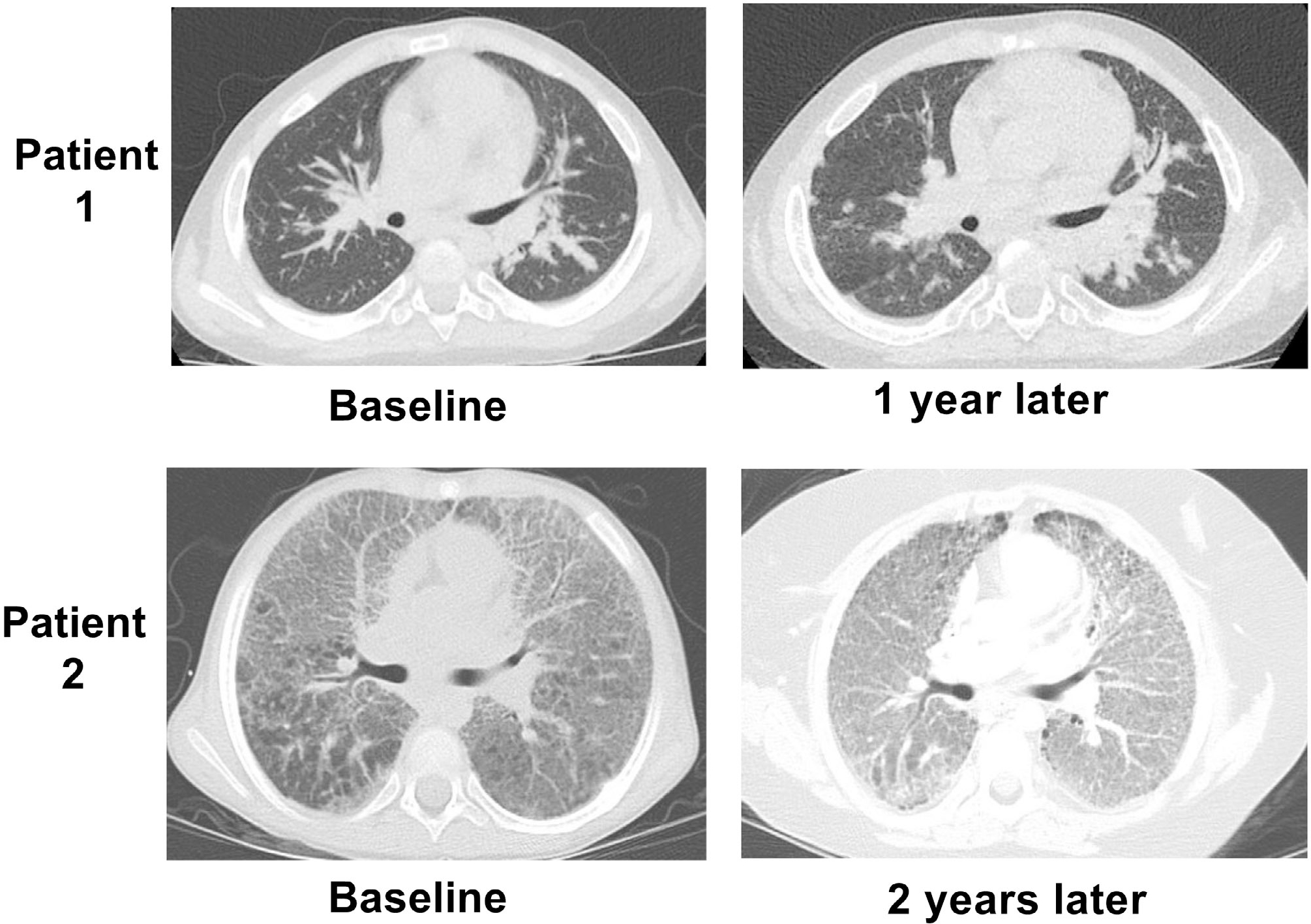
Results: We enrolled 41 patients with SJIA-LD, 85% with at least one episode of macrophage activation syndrome and 41% with adverse reactions to a biologic. Although 93% of patients were alive at last follow-up (median 2.9 years), 37% progressed to requiring chronic oxygen or other ventilator support, and 65% of patients had abnormal overnight oximetry studies, which changed over time. Eighty-four percent of patients carried the HLA-DRB1*15 haplotype, significantly more than patients without LD. Patients with SJIA-LD also showed markedly elevated serum interleukin-18 (IL-18), variable C-X-C motif chemokine ligand 9 (CXCL9), and significantly elevated matrix metalloproteinase 7. Treatment strategies showed variable use of anti-IL-1/6 biologics and addition of other immunomodulatory treatments and lung-directed therapies. We found a broad range of current clinical status independent of time from diagnosis or continued biologic treatment. Multidomain measures of change showed imaging features were the least likely to improve with time.
Conclusion: Patients with SJIA-LD had highly varied courses, with lower mortality than previously reported but frequent hypoxia and requirement for respiratory support. Treatment strategies were highly varied, highlighting an urgent need for focused clinical trials.
© 2023 American College of Rheumatology.
Figures
References
-
- Lee JJY, Schneider R. Systemic juvenile idiopathic arthritis [review]. Pediatr Clin North Am 2018;65:691–709. - PubMed
-
- Woo P, Southwood TR, Prieur AM, et al. Randomized, placebo-controlled, crossover trial of low-dose oral methotrexate in children with extended oligoarticular or systemic arthritis. Arthritis Rheum 2000;43:1849–1857. - PubMed
-
- De Benedetti F, Brunner HI, Ruperto N, et al. ; PRINTO; PRCSG. Randomized trial of tocilizumab in systemic juvenile idiopathic arthritis. N Engl J Med 2012;367:2385–2395. - PubMed
-
- Ruperto N, Brunner HI, Quartier P, et al. ; PRINTO; PRCSG. Two randomized trials of canakinumab in systemic juvenile idiopathic arthritis. N Engl J Med 2012;367:2396–2406. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
