Propensity matched comparison of omaveloxolone treatment to Friedreich ataxia natural history data
- PMID: 37691319
- PMCID: PMC10791025
- DOI: 10.1002/acn3.51897
Propensity matched comparison of omaveloxolone treatment to Friedreich ataxia natural history data
Abstract
Objective: The natural history of Friedreich ataxia is being investigated in a multi-center longitudinal study designated the Friedreich ataxia Clinical Outcome Measures Study (FACOMS). To understand the utility of this study in analysis of clinical trials, we performed a propensity-matched comparison of data from the open-label MOXIe extension (omaveloxolone) to that from FACOMS.
Methods: MOXIe extension patients were matched to FACOMS patients using logistic regression to estimate propensity scores based on multiple covariates: sex, baseline age, age of onset, baseline modified Friedreich Ataxia Rating scale (mFARS) score, and baseline gait score. The change from baseline in mFARS at Year 3 for the MOXIe extension patients compared to the matched FACOMS patients was analyzed as the primary efficacy endpoint using mixed model repeated measures analysis.
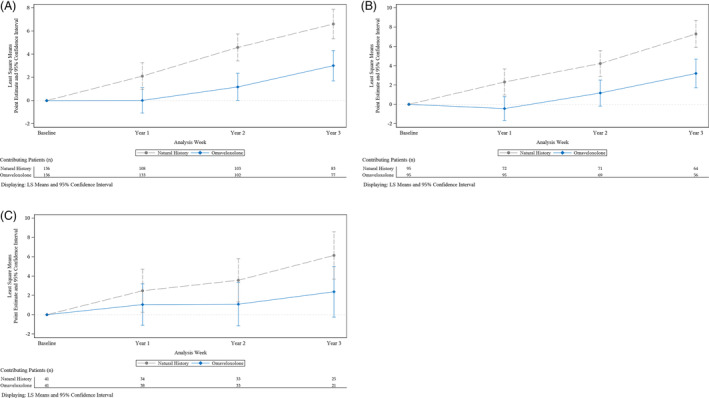
Results: Data from the MOXIe extension show that omaveloxolone provided persistent benefit over 3 years when compared to an untreated, matched cohort from FACOMS. At each year, in all analysis populations, patients in the MOXIe extension experienced a smaller change from baseline in mFARS score than matched FACOMS patients. In the primary pooled population (136 patients in each group) by Year 3, patients in the FACOMS matched set progressed 6.6 points whereas patients treated with omaveloxolone in MOXIe extension progressed 3 points (difference = -3.6; nominal p value = 0.0001).
Interpretation: These results suggest a meaningful slowing of Friedreich ataxia progression with omaveloxolone, and consequently detail how propensity-matched analysis may contribute to understanding of effects of therapeutic agents. This demonstrates the direct value of natural history studies in clinical trial evaluations.
© 2023 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
Lynch D receives grants from FARA, the Muscular Dystrophy Association (MDA), the National Institutes of Health (NIH), Reata Pharmaceuticals, and Retrotope. Rummey C reports research and consultancy fees from FARA, The National Ataxia Foundation (NAF), PTC Therapeutics, Reata Pharmaceuticals, Biohaven, Santhera Pharmaceuticals, and Takeda Pharmaceuticals. Boesch S has received fees for consultancy, advisory boards, and/or honoraria from AbbVie, Ipsen, Reata Pharmaceuticals, Merz Pharma, Stada Arzneimittel, and VICO Therapeutics. Delatycki M, Mariotti C, and Mathews K have received funding from Reata Pharmaceuticals during the study. Mathews K reports personal fees for consultancy from VICO Therapeutics; grants from Takeda and FARA. Giunti P has received grants and consultancy fees from Reata Pharmaceuticals, VICO Therapeutics, and consultancy fees from Triplet Therapeutics, and PTC Therapeutics. Nachbauer W reports advisory and speaker honoraria from Reata Pharmaceuticals. Hoyle C has received grants from Reata Pharmaceuticals, Takeda, and FARA during the conduct of the study; personal fees from Reata Pharmaceuticals and Avexis outside the submitted work. Subramony S H reports grants from Reata Pharmaceuticals, Biohaven Pharmaceuticals, Takeda, PTC Therapeutics, Retrotope, Acceleron Pharmaceuticals, NIH, FDA, MDA, Wyck Foundation, FARA, Stealth, Avidity Biosciences, and Fulcrum Therapeutics. Wilmot G has received grant/research support from Reata Pharmaceuticals, Biohaven Pharmaceuticals, NIH, NAF, and FARA. Weissfeld L is an employee of WCG Clinical, Inc. WCG is a paid consultant for Reata Pharmaceuticals. Zesiewicz T has received compensation for serving on the advisory boards of Boston Scientific, Reata Pharmaceuticals, and Steminent Biotherapeutics; has received personal compensation as senior editor for Neurodegenerative Disease Management and as a consultant for Steminent Biotherapeutics; has received royalty payments as co‐inventor of varenicline for treating imbalance (patent number 9,463,190) and non‐ataxic imbalance (patent number 9,782,404); has received research/grant support as principal investigator/investigator for studies from AbbVie; Biogen; Biohaven Pharmaceuticals; Boston Scientific; Bukwang Pharmaceutical Co, Ltd; Cala Health; Cavion; FARA; Houston Methodist Research Institute; NIH (READISCA U01); Retrotope; and Takeda Development Center Americas. Perlman S reports no conflicts or relevant disclosures. Goldsberry A and Meyer C are employees of Reata Pharmaceuticals. Farmer J is an employee of FARA.
Figures