

Provider adherence to clinical care recommendations for infants and children who died in seven low- and middle-income countries in the Child Health and Mortality Prevention Surveillance (CHAMPS) network
- PMID: 37692079
- PMCID: PMC10484959
- DOI: 10.1016/j.eclinm.2023.102198
Provider adherence to clinical care recommendations for infants and children who died in seven low- and middle-income countries in the Child Health and Mortality Prevention Surveillance (CHAMPS) network
Abstract
Background: Most childhood deaths globally are considered preventable through high-quality clinical care, which includes adherence to clinical care recommendations. Our objective was to describe adherence to World Health Organization recommendations for the management of leading causes of death among children.
Methods: We conducted a retrospective, descriptive study examining clinical data for children aged 1-59 months who were hospitalized and died in a Child Health and Mortality Prevention Surveillance (CHAMPS) catchment, December 2016-June 2021. Catchment areas included: Baliakandi and Faridpur, Bangladesh; Kersa, Haramaya, and Harar, Ethiopia; Kisumu and Siaya, Kenya; Bamako, Mali; Manhiça and Quelimane, Mozambique; Makeni, Sierra Leone; Soweto, South Africa. We reviewed medical records of those who died from lower respiratory tract infections, sepsis, malnutrition, malaria, and diarrheal diseases to determine the proportion who received recommended treatments and compared adherence by hospitalization duration.
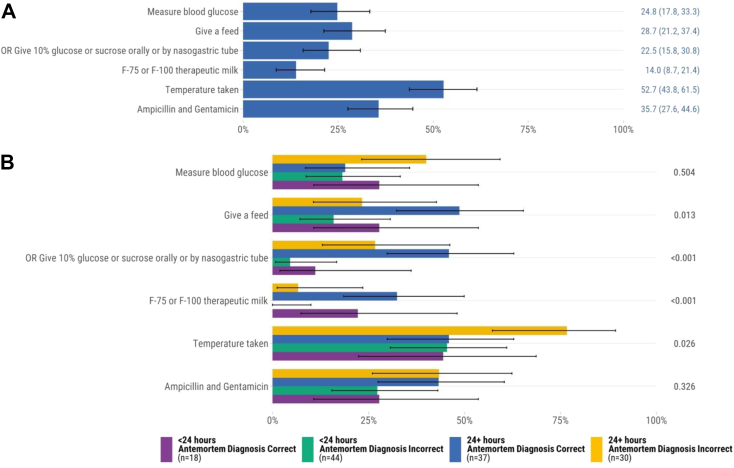
Findings: CHAMPS enrolled 460 hospitalized children who died from the leading causes (median age 12 months, 53.0% male). Median hospital admission was 31 h. There were 51.0% (n = 127/249) of children who died from lower respiratory tract infections received supplemental oxygen. Administration of intravenous fluids for sepsis (15.9%, n = 36/226) and supplemental feeds for malnutrition (14.0%, n = 18/129) were uncommon. There were 51.4% (n = 55/107) of those who died from malaria received antimalarials. Of the 80 children who died from diarrheal diseases, 76.2% received intravenous fluids. Those admitted for ≥24 h more commonly received antibiotics for lower respiratory tract infections and sepsis, supplemental feeds for malnutrition, and intravenous fluids for sepsis than those admitted <24 h.
Interpretation: Provision of recommended clinical care for leading causes of death among young children was suboptimal. Further studies are needed to understand the reasons for deficits in clinical care recommendation adherence.
Funding: Bill & Melinda Gates Foundation.
Keywords: Childhood; Clinical care; Guideline adherence; Mortality.
© 2023 The Author(s).
Conflict of interest statement
CGW received honoraria from the University of St. Andrews for speaking to alumni about CHAMPS and global health work. JAGS reports receiving funding from the Wellcome Trust, UK FCDO, European Union, and the National Institute for Health Research. SM has received grants from the Bill & Melinda Gates Foundation, GSK, Pfizer, Minervax, Novavax, Providence, Gritstone, and ImmunityBio. SM has received honoraria from GSK for lecturing. CGW and SM report serving on data safety monitoring boards for SPEAC (CGW) and PATH and CAPRISA (SM). All other investigators declare no competing interests.
Figures




References
-
- GBD 2019 Demographics Collaborators Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1160–1203. - PMC - PubMed
-
- Liu L., Oza S., Hogan D., et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385:430–440. - PubMed
-
- World Health Organization Child mortality (under 5 years) 2022. https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-ch...
-
- World Bank Mortality rate, under-5 (per 1,000 live births) - South Asia. https://data.worldbank.org/indicator/SH.DYN.MORT?end=2021&locations=8S&m...
Grants and funding
LinkOut - more resources
Full Text Sources
