

Evolution of a globally unique SARS-CoV-2 Spike E484T monoclonal antibody escape mutation in a persistently infected, immunocompromised individual
- PMID: 37692895
- PMCID: PMC10491860
- DOI: 10.1093/ve/veac104
Evolution of a globally unique SARS-CoV-2 Spike E484T monoclonal antibody escape mutation in a persistently infected, immunocompromised individual
Abstract
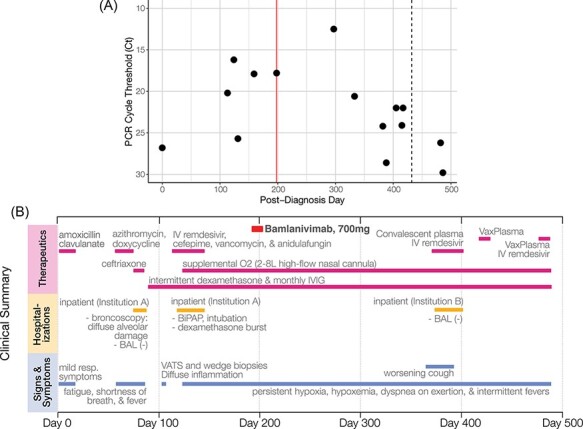
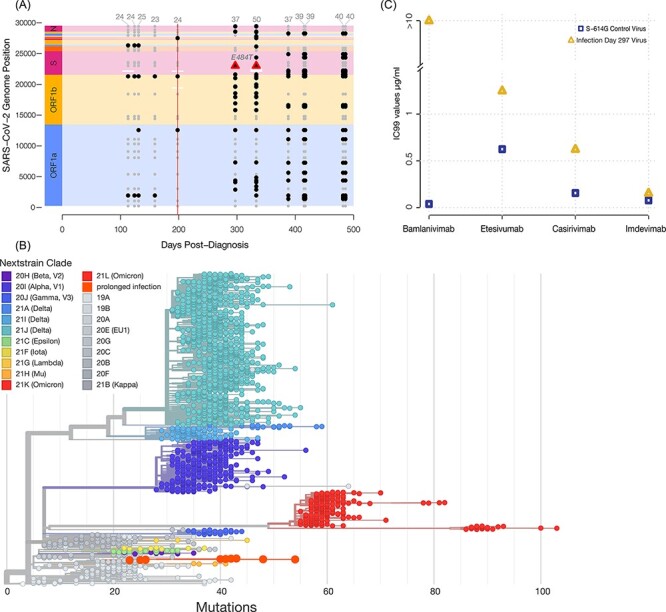
Prolonged infections in immunocompromised individuals may be a source for novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) variants, particularly when both the immune system and antiviral therapy fail to clear the infection and enable within-host evolution. Here we describe a 486-day case of SARS-CoV-2 infection in an immunocompromised individual. Following monotherapy with the monoclonal antibody Bamlanivimab, the individual's virus acquired resistance, likely via the earliest known occurrence of Spike amino acid variant E484T. Recently, E484T has arisen again as a derivative of E484A in the Omicron Variant of Concern, supporting the hypothesis that prolonged infections can give rise to novel variants long before they become prevalent in the human population.
Keywords: SARS-CoV-2; Spike protein; antibody escape; immunocompromised host; novel mutation; prolonged infection.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
We declare no conflicts of interest.
Figures
References
-
- BBMap . [cited 13 Dec 2021]. <https://sourceforge.net/projects/bbmap/>.
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
