

Pulmonary Assessment of the Liver Transplant Recipient
- PMID: 37693254
- PMCID: PMC10483013
- DOI: 10.1016/j.jceh.2023.04.003
Pulmonary Assessment of the Liver Transplant Recipient
Abstract
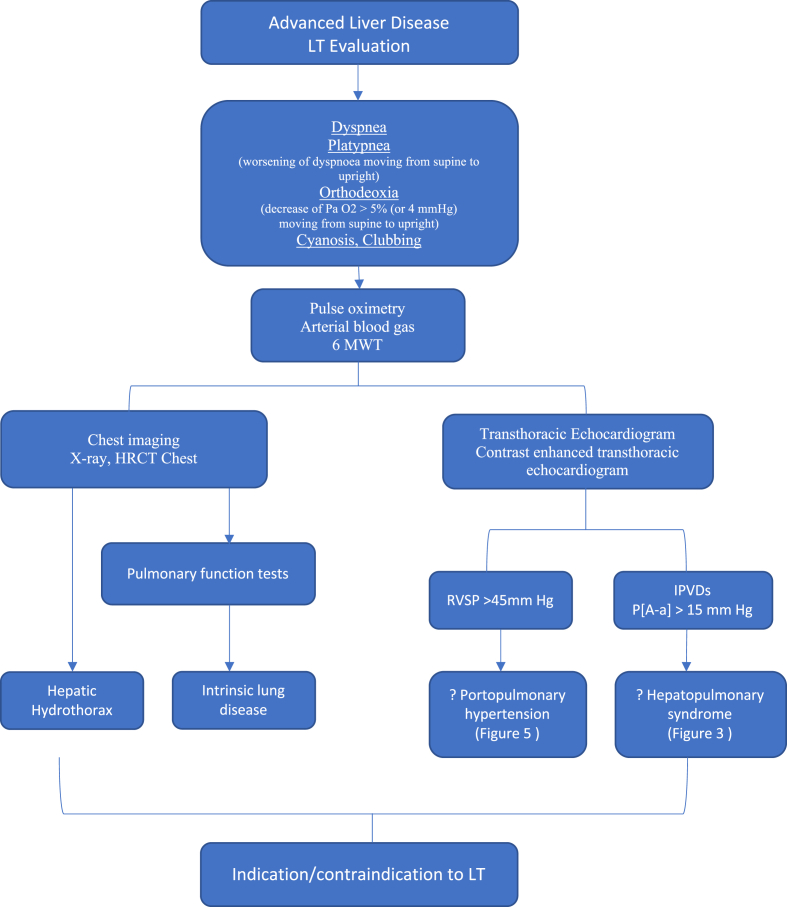
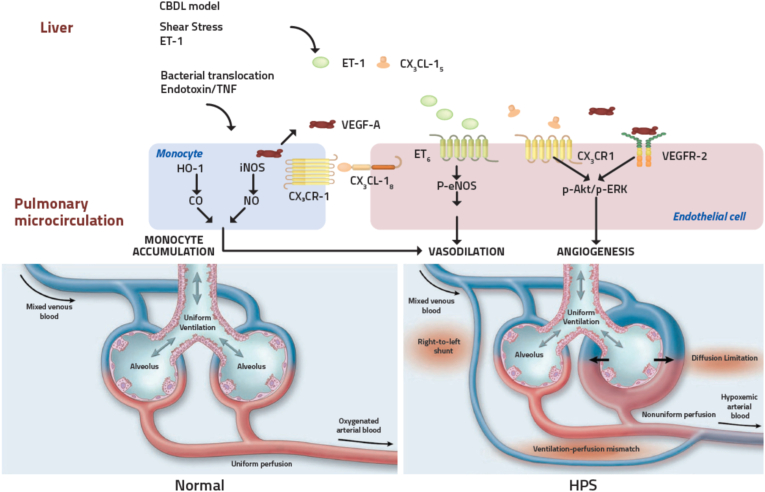
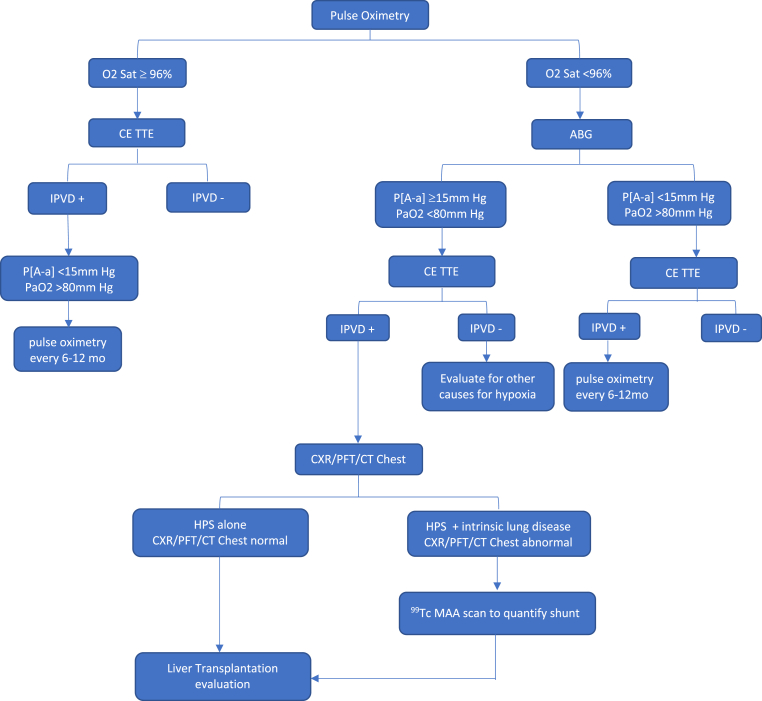
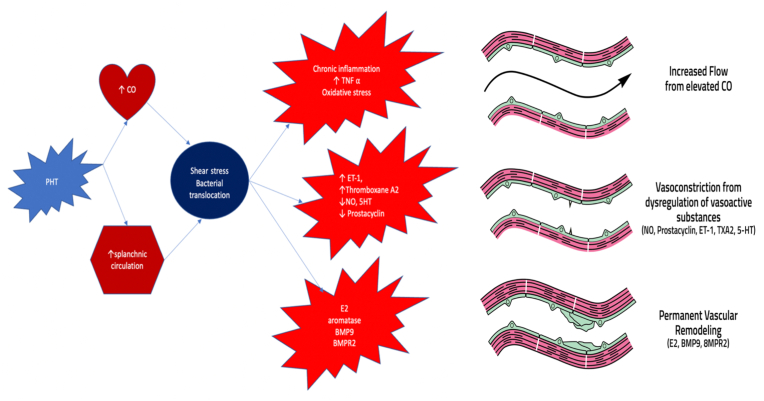
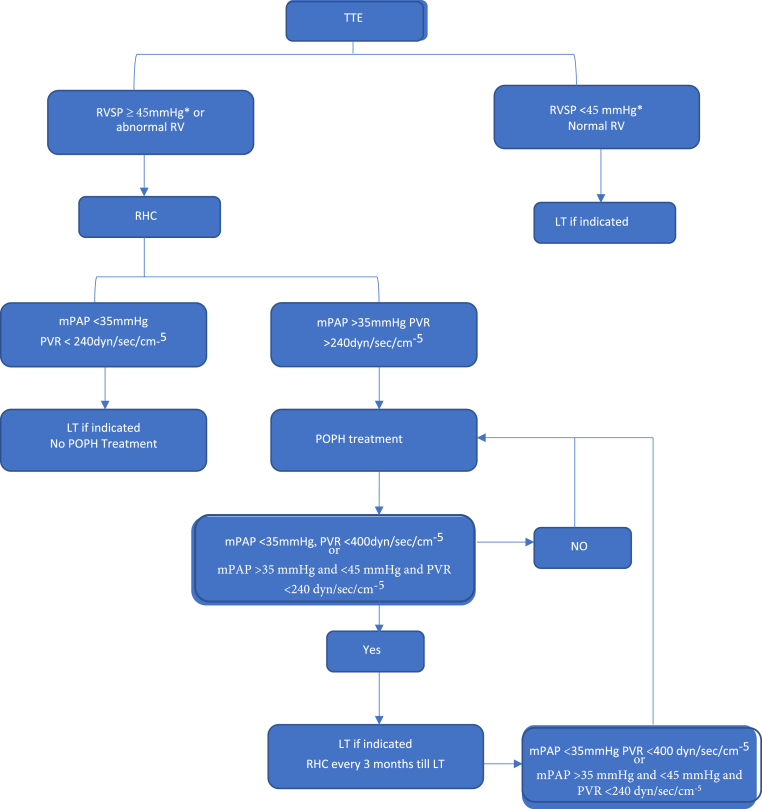
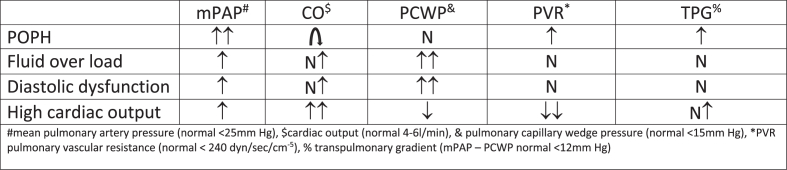
Respiratory symptoms and hypoxemia can complicate chronic liver disease and portal hypertension. Various pulmonary disorders affecting the pleura, lung parenchyma, and pulmonary vasculature are seen in end-stage liver disease, complicating liver transplantation (LT). Approximately 8% of cirrhotic patients in an intensive care unit develop severe pulmonary problems. These disorders affect waiting list mortality and posttransplant outcomes. A thorough history, physical examination, and appropriate laboratory tests help diagnose and assess the severity to risk stratify pulmonary diseases before LT. Hepatopulmonary syndrome (HPS), portopulmonary hypertension (POPH), and hepatic hydrothorax (HH) are respiratory consequences specific to cirrhosis and portal hypertension. HPS is seen in 5-30% of cirrhosis cases and is characterized by impaired oxygenation due to intrapulmonary vascular dilatations and arteriovenous shunts. Severe HPS is an indication of LT. The majority of patients with HPS resolve their hypoxemia after LT. When pulmonary arterial hypertension occurs in patients with portal hypertension, it is called POPH. All other causes of pulmonary arterial hypertension should be ruled out before labeling as POPH. Since severe POPH (mean pulmonary artery pressure [mPAP] >50 mm Hg) is a relative contraindication for LT, it is crucial to screen for POPH before LT. Those with moderate POPH (mPAP >35 mm Hg), who improve with medical therapy, will benefit from LT. A transudative pleural effusion called hepatic hydrothorax (HH) is seen in 5-10% of people with cirrhosis. Refractory cases of HH benefit from LT. In recent years, increasing clinical expertise and advances in the medical field have resulted in better outcomes in patients with moderate to severe pulmonary disorders, who undergo LT.
Keywords: hepatic hydrothorax; hepatopulmonary syndrome; liver transplantation; portopulmonary hypertension; pulmonary artery hypertension.
© 2023 Indian National Association for Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Pulmonary complications in chronic liver disease.Hepatology. 2014 Apr;59(4):1627-37. doi: 10.1002/hep.26745. Epub 2014 Feb 25. Hepatology. 2014. PMID: 24089295 Review.
-
Pulmonary Complications of Portal Hypertension.Clin Liver Dis. 2024 Aug;28(3):467-482. doi: 10.1016/j.cld.2024.03.005. Epub 2024 May 1. Clin Liver Dis. 2024. PMID: 38945638 Review.
-
Hepatopulmonary Syndrome and Portopulmonary Hypertension: Management in Liver Transplantation in the Horizon 2020.Transplant Proc. 2020 Jun;52(5):1503-1506. doi: 10.1016/j.transproceed.2020.02.057. Epub 2020 Apr 9. Transplant Proc. 2020. PMID: 32278579
-
Recent advances in the approach to hepatopulmonary syndrome and portopulmonary hypertension.Acta Gastroenterol Belg. 2021 Jan-Mar;84(1):95-99. doi: 10.51821/84.1.200. Acta Gastroenterol Belg. 2021. PMID: 33639700 Review.
-
Hepatopulmonary Syndrome and Portopulmonary Hypertension: Current Status and Implications for Liver Transplantation.Curr Hepatol Rep. 2020 Sep;19(3):174-185. doi: 10.1007/s11901-020-00532-y. Epub 2020 Jul 11. Curr Hepatol Rep. 2020. PMID: 32905452 Free PMC article.
References
-
- Machicao V.I., Balakrishnan M., Fallon M.B. Pulmonary complications in chronic liver disease. Hepatology. 2014;59:1627–1637. - PubMed
-
- Fallon M.B., Abrams G.A. Pulmonary dysfunction in chronic liver disease. Hepatology. 2000;32:859–865. - PubMed
-
- Krowka M.J., Cortese D.A. Hepatopulmonary syndrome. Current concepts in diagnostic and therapeutic considerations. Chest. 1994;105:1528–1537. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
