

doi: 10.1016/j.jceh.2023.03.003.
Epub 2023 Mar 20.
Secondary Budd-Chiari Syndrome due to Hepatic Tuberculosis in a Pediatric Patient Managed by Left Hepatic Vein Stenting
Affiliations
- PMID: 37693276
- PMCID: PMC10482985
- DOI: 10.1016/j.jceh.2023.03.003
Item in Clipboard
Secondary Budd-Chiari Syndrome due to Hepatic Tuberculosis in a Pediatric Patient Managed by Left Hepatic Vein Stenting
J Clin Exp Hepatol.
2023 Sep-Oct.
No abstract available
Figures

(a) USG shows an enlarged left lobe with heterogeneous parenchymal echotexture, an ill-defined iso to hyperechoic mass (black arrow) involving LHV; (b, c) Colour Doppler shows monophasic flow in LHV, s/o LHV stenosis with multiple tiny intrahepatic veno-venous collaterals.

(a) Axial CECT image shows atrophied right lobe, multiple discrete and conglomerated hypoechoic lesions in the right and caudate lobe (black arrows) with enlarged and congested left lobe (white arrow); (b) Associated findings include multiple enlarged and necrotic retroperitoneal lymphadenopathy with few of them showing calcifications (white circle b).
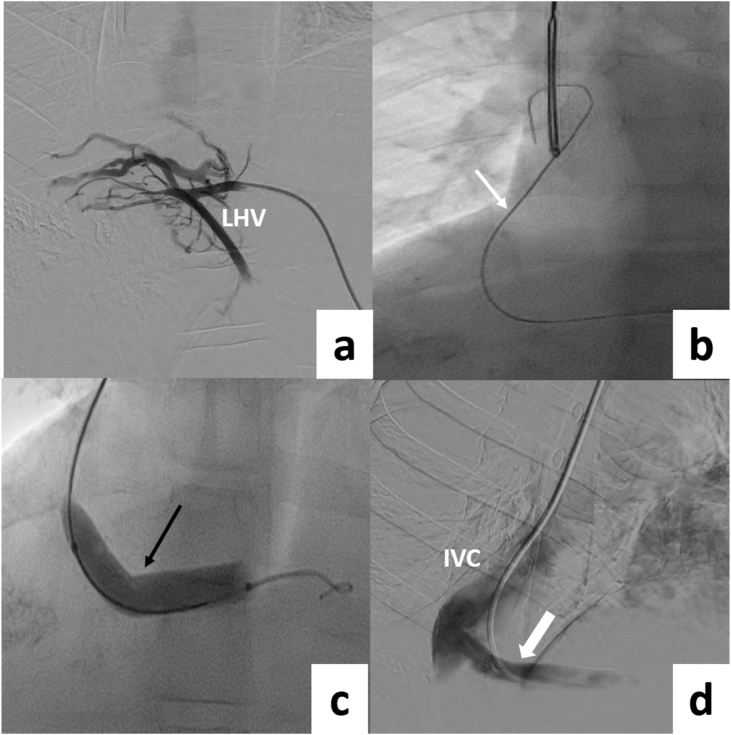
(a) Left hepatic venogram following percutaneous transhepatic access shows long segment occlusion of LHV with multiple collaterals around the LHV and non-opacification of IVC; (b) Stricture was negotiated, and a 0.018″ guidewire (white arrow) was snared through transjugular route to obtain a through and through access. (c) The stricture was serially dilated using a 4–10 mm balloon; (d) Venogram after stent deployment (black arrow) shows free flow into the IVC (white arrow).

(a, b) Follow-up USG at one month shows the stent in situ with the flow within the stent.
References
-
- Victor S., Jayanthi V., Madanagopalan N. Budd Chiari syndrome in a child with hepatic tuberculosis. Indian Heart J. 1989 Jul-Aug;41:279. PMID: 2807366. - PubMed
-
- Gomber S., Khalil A., Vij J.C., Bahl V.K., Kapoor R., Saini L. Budd Chiari syndrome in a child with hepatic tuberculosis. Indian Heart J. 1986 May-Jun;38:226–229. PMID: 3557528. - PubMed
-
- Mukund A., Mittal K., Mondal A., Sarin S.K. Anatomic recanalization of hepatic vein and inferior vena cava versus direct intrahepatic portosystemic shunt creation in Budd-Chiari syndrome: overall outcome and midterm transplant-free survival. J Vasc Intervent Radiol. 2018 Jun;29:790–799. doi: 10.1016/j.jvir.2018.01.781. Epub 2018 Apr 25. PMID: 29705227. - DOI - PubMed
LinkOut - more resources
Full Text Sources
