

Miller Fisher syndrome: an updated narrative review
- PMID: 37693761
- PMCID: PMC10484709
- DOI: 10.3389/fneur.2023.1250774
Miller Fisher syndrome: an updated narrative review
Abstract
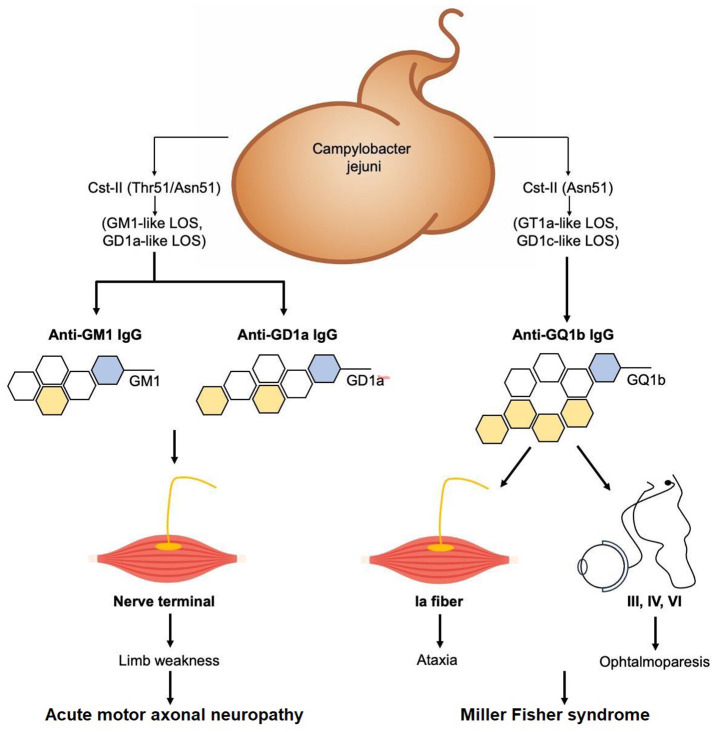
Introduction: Miller Fisher syndrome (MFS) is considered a rare variant of Guillain-Barré syndrome (GBS), a group of acute-onset immune-mediated neuropathies characterized by the classic triad of ataxia, areflexia, and ophthalmoparesis. The present review aimed to provide a detailed and updated profile of all aspects of the syndrome through a collection of published articles on the subject, ranging from the initial description to recent developments related to COVID-19.
Methods: We searched PubMed, Scopus, EMBASE, and Web of Science databases and gray literature, including references from the identified studies, review studies, and conference abstracts on this topic. We used all MeSH terms pertaining to "Miller Fisher syndrome," "Miller Fisher," "Fisher syndrome," and "anti-GQ1b antibody."
Results: An extensive bibliography was researched and summarized in the review from an initial profile of MFS since its description to the recent accounts of diagnosis in COVID-19 patients. MFS is an immune-mediated disease with onset most frequently following infection. Anti-ganglioside GQ1b antibodies, detected in ~85% of patients, play a role in the pathogenesis of the syndrome. There are usually no abnormalities in MFS through routine neuroimaging. In rare cases, neuroimaging shows nerve root enhancement and signs of the involvement of the central nervous system. The most consistent electrophysiological findings in MFS are reduced sensory nerve action potentials and absent H reflexes. Although MFS is generally self-limited and has excellent prognosis, rare recurrent forms have been documented.
Conclusion: This article gives an updated narrative review of MFS with special emphasis on clinical characteristics, neurophysiology, treatment, and prognosis of MFS patients.
Keywords: Miller Fisher; Miller Fisher syndrome; anti-GQ1b antibody; ataxia; ophthalmoparesis.
Copyright © 2023 Noioso, Bevilacqua, Acerra, Della Valle, Serio, Vinciguerra, Piscosquito, Toriello, Barone and Iovino.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Lolekha P, Phanthumchinda K. Miller-Fisher syndrome at King Chulalongkorn Memorial Hospital. J Med Assoc Thail Chotmaihet Thangphaet. (2009) 92:471–7. - PubMed
-
- Clinical E, Neurology EP. Guillain-Barré syndrome variants in Emilia-Romagna, Italy, 1992-3: incidence, clinical features, and prognosis. Emilia-Romagna Study Group on clinical and epidemiological problems in neurology. J Neurol Neurosurg Psychiatry. (1998) 65:218–24. 10.1136/jnnp.65.2.218 - DOI - PMC - PubMed
-
- Téllez-Zenteno JF, Jacinto-Tinajero JC, Avila-Funes A, García-Ramos G, Negrete-Pulido O, Sentíes-Madrid H. Guillain-Barre syndrome. Experience in a third level hospital. Rev Investig Clin Organo Hosp Enfermedades Nutr. (2001) 53:311–4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources