

An assessment of childhood cancer care services in India - gaps, challenges and the way forward
- PMID: 37694177
- PMCID: PMC10485780
- DOI: 10.1016/j.lansea.2023.100235
An assessment of childhood cancer care services in India - gaps, challenges and the way forward
Abstract
Background: Childhood cancers are emerging as an essential concern in India where there is lack of a specific programme component or policy to address childhood cancer control. There is limited information on the status and quality of childhood cancer care services in India. This paper describes the childhood cancer care services available at secondary and tertiary-level hospitals in India through a cross sectional study design.
Methods: The survey was conducted in 137 tertiary-level and 92 secondary-level hospitals in 26 states and 4 Union Territories (UTs), ensuring a uniform representation of public and private care hospitals. The study tool collected data on the organisational infrastructure, type of oncology services, health workforce, equipment, treatment and referral protocols, and treatment guidelines. Descriptive statistics was used to primarily present the health service status and data on childhood cancer care services in proportions and mean.
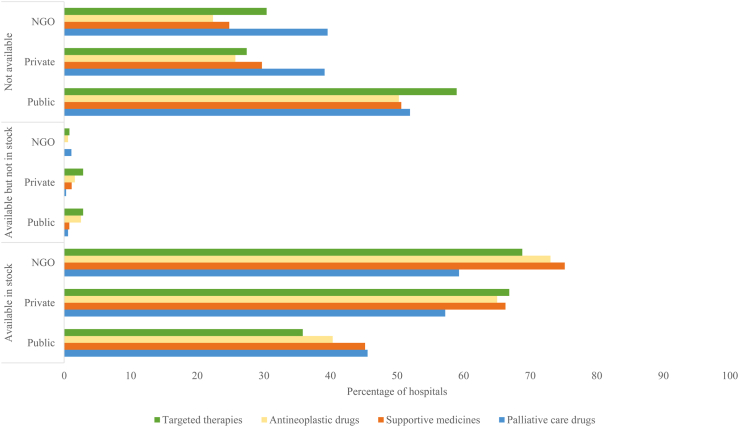
Findings: A dedicated pediatric oncology department was available in 41.6% of the public, 48.6% of private, and 64% Non Government Organization (NGO) managed tertiary-level hospitals. In 36 (39%) of the 92 hospitals providing secondary care, childhood cancer care was provided. The availability of bone (41.5%) and positron emission tomography (PET) scans (25.9%) was lower in public tertiary hospitals, whereas histopathology, computerised tomography (CT scan), and magnetic resonance imaging (MRI) were lower in public secondary hospitals than private and NGO managed hospitals for the corresponding level of care. Most tertiary hospitals had the required supportive care facilities except for play therapy and hospice care. Less than 50% of the public tertiary hospitals had stocks of the four categories of cancer-treating drugs and essential infrastructure for radiotherapy and chemotherapy. Most secondary-level hospitals not treating childhood cancer had referral linkages with tertiary hospitals.
Interpretation: The situational analysis of childhood cancer care services in India showed the concentration of availability of childhood cancer care services at the tertiary level of health care. There were gaps in the availability of specialised pediatric oncology care in all the tertiary hospitals. The availability of childhood cancer care services was higher in private and NGO-managed hospitals than in public hospitals. Integration of childhood cancer as a part of the national cancer control response should be taken up as a matter of priority. The need of the hour is to formulate a childhood cancer policy that will enable timely access to care universally.
Funding: World Health Organization, India provided funding and technical support.
Keywords: Care; Childhood cancer; Health services; India.
© 2023 The Author(s).
Conflict of interest statement
None to declare.
Figures


References
-
- Bhakta N., Force L.M., Allemani C., et al. Childhood cancer burden: a review of global estimates. Lancet Oncol. 2019;20:e42–e53. - PubMed
-
- Institute for Health Metrics and Evaluation (IHME) University of Washington, IHME; Seattle: 2017. GBD compare.https://vizhub.healthdata.org/gbd-compare/ Available on:
-
- Gatta G., Botta L., Rossi S., et al. Childhood cancer survival in Europe 1999–2007: results of EUROCARE-5—a population-based study. Lancet Oncol. 2014;15:35–47. - PubMed
LinkOut - more resources
Full Text Sources
