

Delirium is associated with loss of feedback cortical connectivity
- PMID: 37695013
- PMCID: PMC10840828
- DOI: 10.1002/alz.13471
Delirium is associated with loss of feedback cortical connectivity
Abstract
Introduction: Post-operative delirium (POD) is associated with increased morbidity and mortality but is bereft of treatments, largely due to our limited understanding of the underlying pathophysiology. We hypothesized that delirium reflects a disturbance in cortical connectivity that leads to altered predictions of the sensory environment.
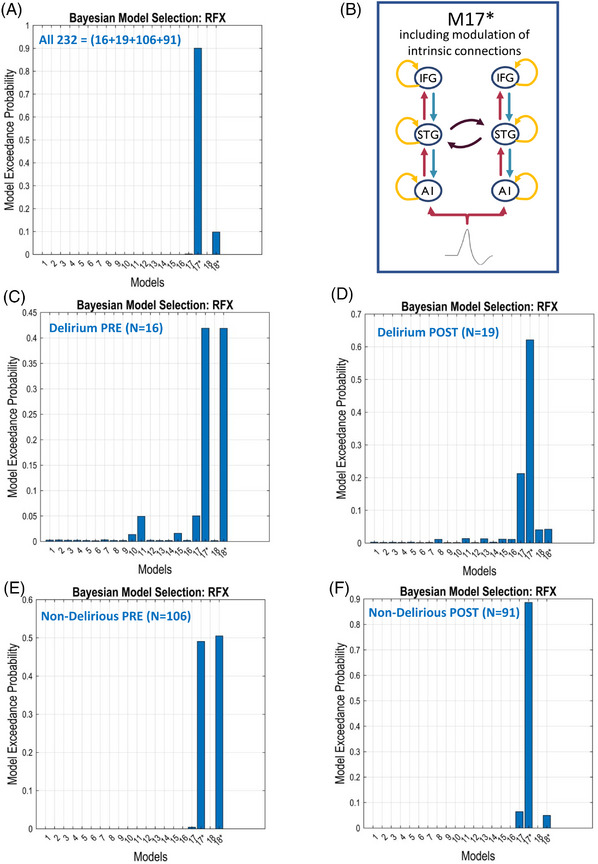
Methods: High-density electroencephalogram recordings during an oddball auditory roving paradigm were collected from 131 patients. Dynamic causal modeling (DCM) analysis facilitated inference about the neuronal connectivity and inhibition-excitation dynamics underlying auditory-evoked responses.
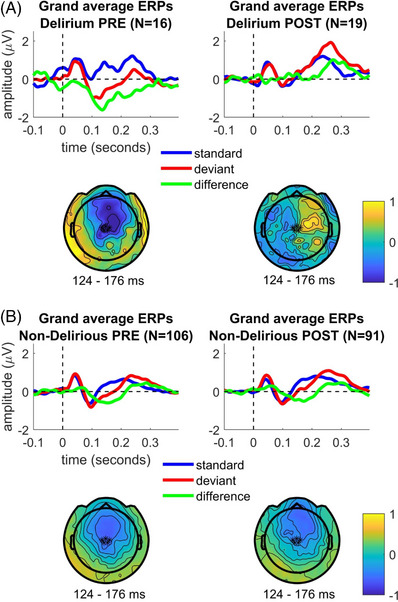
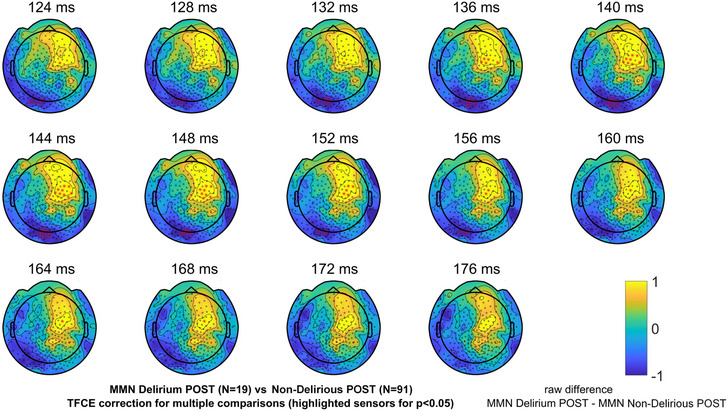
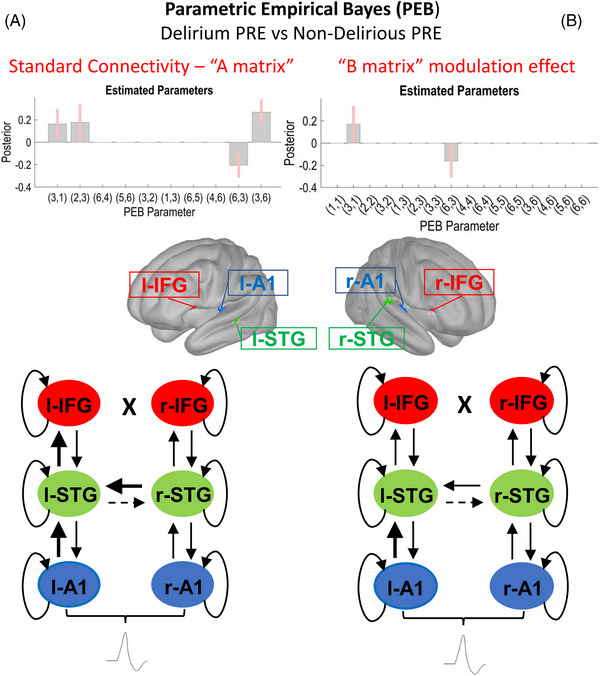
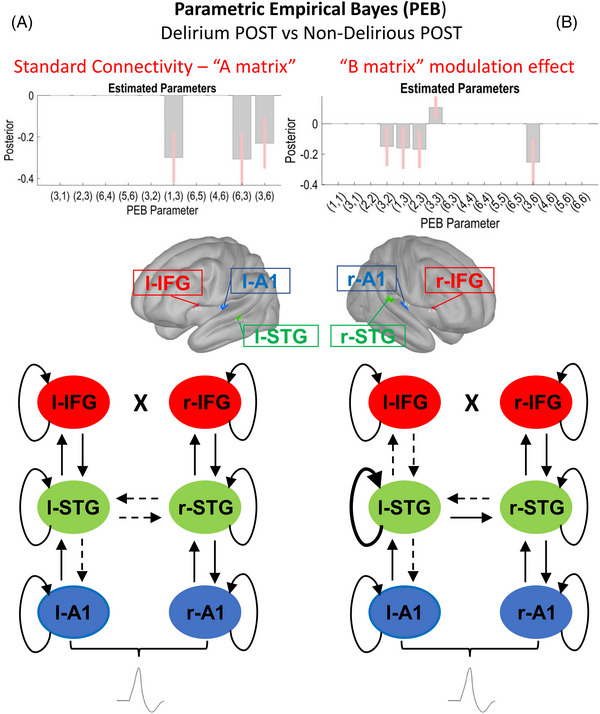
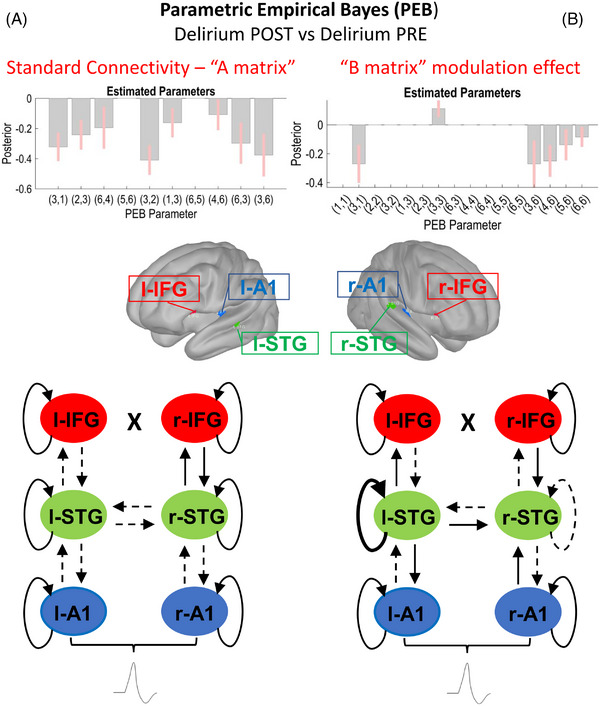
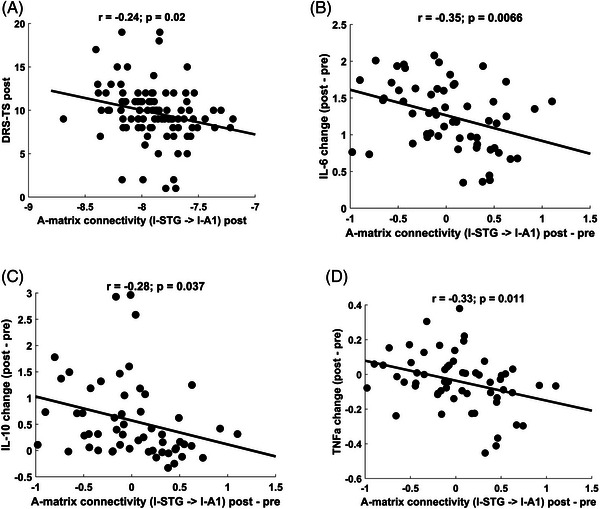
Results: Mismatch negativity amplitudes were smaller in patients with POD. DCM showed that delirium was associated with decreased left-sided superior temporal gyrus (l-STG) to auditory cortex feedback connectivity. Feedback connectivity also negatively correlated with delirium severity and systemic inflammation. Increased inhibition of l-STG, with consequent decreases in feed-forward and feed-back connectivity, occurred for oddball tones during delirium.
Discussion: Delirium is associated with decreased feedback cortical connectivity, possibly resulting from increased intrinsic inhibitory tone.
Highlights: Mismatch negativity amplitude was reduced in patients with delirium. Patients with postoperative delirium had increased feedforward connectivity before surgery. Feedback connectivity was diminished from left-side superior temporal gyrus to left primary auditory sensory area during delirium. Feedback connectivity inversely correlated with inflammation and delirium severity.
Keywords: auditory roving oddball paradigm; delirium; dynamic causal modeling; event-related potentials; evoked response potentials; high-density electroencephalogram; mismatch negativity; postoperative delirium; predictive coding framework.
© 2023 The Authors. Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
The authors declare no conflicts of interest pertinent to this manuscript. Author disclosures are available in the supporting information.
Figures
References
-
- Pereira JV, Aung Thein MZ, Nitchingham A, Caplan GA. Delirium in older adults is associated with development of new dementia: a systematic review and meta‐analysis. Int J Geriatr Psychiatry. 2021;36(7):993‐1003. - PubMed
-
- Sanders RD, Pandharipande PP, Davidson AJ, Ma D, Maze M. Anticipating and managing postoperative delirium and cognitive decline in adults. BMJ. 2011;343:d4331. - PubMed
-
- Sanders RD. Hypothesis for the pathophysiology of delirium: role of baseline brain network connectivity and changes in inhibitory tone. Med Hypotheses. 2011;77:140‐143. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
