

Usefulness of tumor perfusion on cone-beam CT after hepatic arterial infusion port implantation for evaluating tumor response to hepatic arterial infusion chemotherapy in hepatocellular carcinoma treatment
- PMID: 37695260
- PMCID: PMC10679554
- DOI: 10.4274/dir.2023.232311
Usefulness of tumor perfusion on cone-beam CT after hepatic arterial infusion port implantation for evaluating tumor response to hepatic arterial infusion chemotherapy in hepatocellular carcinoma treatment
Abstract
Purpose: To compare tumor perfusion on cone-beam computed tomography (CBCT) after hepatic artery infusion port implantation with the tumor response to hepatic arterial infusion chemotherapy (HAIC) in patients with hepatocellular carcinoma (HCC).
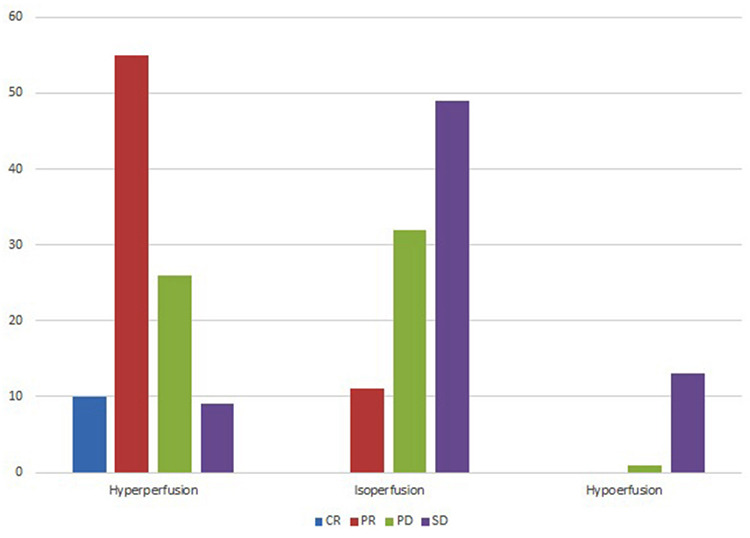
Methods: This retrospective study was conducted in patients with advanced HCC treated with HAIC from 2015 to 2020. We performed CBCT with contrast injection via a port on the day following implantation. We classified tumor perfusion on CBCT into three groups: hyperperfusion, isoperfusion, and hypoperfusion. We also evaluated tumor response to HAIC on follow-up images using RECIST 1.1 and compared it with tumor perfusion on CBCT.
Results: This study included 206 tumors in 193 patients (mean: 60.5 years) with HCC. There were 100 hyperperfusion tumors (48.5%), 92 isoperfusion tumors (44.7%), and 14 hypoperfusion tumors (6.8%). The tumor response to HAIC included 10 tumors with a complete response (CR) (4.9%), 66 tumors with a partial response (32%), 60 tumors with stable disease (29.1%), and 70 tumors with progressive disease (34%). Hyperperfusion tumors had a 65% objective response rate (ORR) and a 92% disease control rate (DCR). Isoperfusion tumors had a 12% ORR and a 46.8% DCR, while hypoperfusion tumors had a 0% ORR and a 7.1% DCR. A CR was shown only in hyperperfusion tumors. The ORR and DCR of the three groups were different, with statistical significance (P < 0.001).
Conclusion: Hyperperfusion tumors on CBCT showed a better tumor response to HAIC, with a 65% ORR in patients with HCC. Tumor perfusion on CBCT after implantation of the hepatic arterial infusion port was associated with the tumor response to HAIC.
Keywords: Cone-beam CT; hepatic arterial infusion chemotherapy; hepatocellular carcinoma; tumor perfusion; tumor response.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures

Similar articles
-
Evaluation of intrahepatic perfusion on fusion imaging using a combined CT/SPECT system: influence of anatomic variations on hemodynamic modification before installation of implantable port systems for hepatic arterial infusion chemotherapy.Cardiovasc Intervent Radiol. 2007 May-Jun;30(3):383-91. doi: 10.1007/s00270-006-0015-x. Cardiovasc Intervent Radiol. 2007. PMID: 17225972
-
Tumor-feeding artery diameter reduction is associated with improved short-term effect of hepatic arterial infusion chemotherapy plus lenvatinib treatment.World J Gastroenterol. 2022 Jul 14;28(26):3232-3242. doi: 10.3748/wjg.v28.i26.3232. World J Gastroenterol. 2022. PMID: 36051348 Free PMC article.
-
Pathological complete response by advanced hepatocellular carcinoma with massive macrovascular invasion to hepatic arterial infusion chemotherapy: a case report.World J Surg Oncol. 2019 Dec 26;17(1):229. doi: 10.1186/s12957-019-1772-8. World J Surg Oncol. 2019. PMID: 31878937 Free PMC article.
-
Systematic review of hepatic arterial infusion chemotherapy versus sorafenib in patients with hepatocellular carcinoma with portal vein tumor thrombosis.J Gastroenterol Hepatol. 2020 Aug;35(8):1277-1287. doi: 10.1111/jgh.15010. Epub 2020 Mar 3. J Gastroenterol Hepatol. 2020. PMID: 32052876
-
Sorafenib versus hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma: a systematic review and meta-analysis.Jpn J Clin Oncol. 2019 Sep 1;49(9):845-855. doi: 10.1093/jjco/hyz069. Jpn J Clin Oncol. 2019. PMID: 31063184
Cited by
-
Predictive value of baseline CT imaging features combined with serum biomarkers for neoadjuvant chemotherapy response in adenocarcinoma of the gastroesophageal junction.Am J Cancer Res. 2025 Apr 25;15(4):1955-1971. doi: 10.62347/XLSV6197. eCollection 2025. Am J Cancer Res. 2025. PMID: 40371150 Free PMC article.
-
Hepatic arterial infusion chemotherapy for hepatocellular carcinoma refractory to transarterial chemoembolization: exploring the influence of prior transarterial chemoembolization and additional transarterial chemoembolization on survival outcomes.J Gastrointest Oncol. 2024 Apr 30;15(2):721-729. doi: 10.21037/jgo-23-1006. Epub 2024 Apr 26. J Gastrointest Oncol. 2024. PMID: 38756625 Free PMC article.
References
-
- Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. - PubMed
-
- Lyu N, Kong Y, Mu L, et al. Hepatic arterial infusion of oxaliplatin plus fluorouracil/leucovorin vs. sorafenib for advanced hepatocellular carcinoma. J Hepatol. 2018;69(1):60–69. - PubMed
-
- Kudo M, Ueshima K, Yokosuka O, et al. Sorafenib plus low-dose cisplatin and fluorouracil hepatic arterial infusion chemotherapy versus sorafenib alone in patients with advanced hepatocellular carcinoma (SILIUS): a randomised, open label, phase 3 trial. Lancet Gastroenterol Hepatol. 2018;3(6):424–432. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
