

Electrocardiographic characteristics of newborns with ventricular septal defects: a Copenhagen Baby Heart Study
- PMID: 37695415
- PMCID: PMC10640423
- DOI: 10.1007/s00431-023-05187-7
Electrocardiographic characteristics of newborns with ventricular septal defects: a Copenhagen Baby Heart Study
Abstract
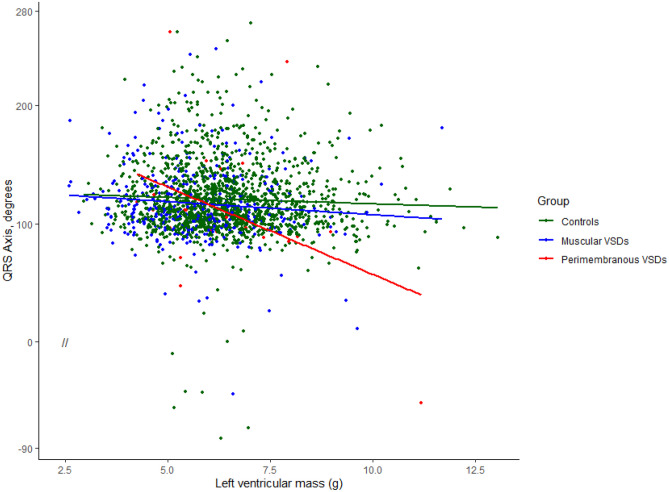
Ventricular septal defects (VSD) represent the most common congenital heart defect in newborns. We assessed the electrocardiographic characteristics of newborns with VSDs in a general population sample. The Copenhagen Baby Heart Study is a prospective population-based cohort study offering cardiac evaluation of newborns. Echocardiograms and electrocardiograms were obtained within 30 days after birth and systematically analysed. A VSD was identified in 530 newborns (mean age 11 ± 7 days, 42% boys). Newborns with VSDs had a more left-shifted QRS axis (116 ± 34 vs. 120 ± 3°, p = 0.02), and a higher S-wave amplitude in V1 (721 ± 584 vs. 636 ± 549 µV, p = 0.001) than controls. The largest differences were found in newborns with large or perimembraneous VSDs with a higher frequency of left axis deviation, higher S-wave amplitudes in V1, and higher R- and S-wave amplitudes in V6 compared with controls. R-waves in V1 and V6 were significantly associated to left ventricular mass, whereas S-waves in V1 and V6 were dependent on left ventricular end-diastolic diameter on echocardiography. Conclusion: Newborns with VSDs showed significant differences in QRS axis, and R- and S-wave precordial amplitudes compared to matched controls. Perimembranous and large VSDs had the greatest effect on the neonatal ECG. What is Known: • Ventricular septal defects in newborns are prevalent and may affect cardiac function and structure. What is New: • The Copenhagen Baby Heart Study is the largest study including a cohort of unselected newborns undergoing postnatal cardiac examination. • We found that newborns with VSD showed significant electrocardiographic differences depending on size and type of VSD compared with healthy newborns.
Keywords: CBHS; Congenital heart defect; Copenhagen Baby Heart Study; Ventricular septal defect.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Dolk H, Loane M, Garne E, European Surveillance of Congenital Anomalies (EUROCAT) Working Group. Congenital heart defects in Europe: prevalence and perinatal mortality to 2005. Circulation. 2000;2011(123):841–849. - PubMed
-
- Dushane JW, Weidman WH, Brandenburg RO, Kirklin JW (1960) The electrocardiogram in children with ventricular septal defect and severe pulmonary hypertension. Correlation with response of pulmonary arterial pressure to surgical repair. Circulation 22:49–54 - PubMed
-
- Schwartz PJ, Garson A, Paul T, Stramba-Badiale M, Vetter VL, Wren C (2002) European Society of Cardiology. Guidelines for the interpretation of the neonatal electrocardiogram. A task force of the European Society of Cardiology. Eur Heart J 23:1329–1344 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
