Pharmacotherapy for Dravet Syndrome: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
- PMID: 37695433
- PMCID: PMC10582139
- DOI: 10.1007/s40265-023-01936-y
Pharmacotherapy for Dravet Syndrome: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Abstract
Background: Dravet syndrome (DS) is a severe developmental and epileptic encephalopathy characterized by drug-resistant, lifelong seizures. The management of seizures in DS has changed in recent years with the approval of new antiseizure medications (ASMs).
Objective: The aim of this study was to estimate the comparative efficacy and tolerability of the ASMs for the treatment of seizures associated with DS using a network meta-analysis (NMA).
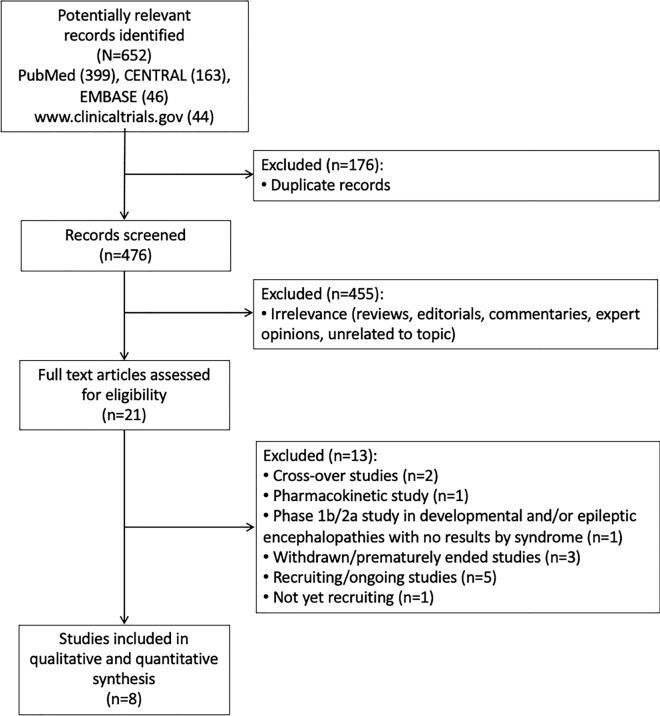
Methods: Studies were identified by conducting a systematic search (week 4, January 2023) of the MEDLINE (accessed by PubMed), EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), and US National Institutes of Health Clinical Trials Registry ( http://www.
Clinicaltrials: gov ) databases. Any randomized, controlled, double- or single-blinded, parallel-group study comparing at least one ASM therapy against placebo, another ASM, or a different dose of the same ASM in participants with a diagnosis of DS was identified. The efficacy outcomes were the proportions of participants with ≥ 50% (seizure response) and 100% reduction (seizure freedom) in baseline convulsive seizure frequency during the maintenance period. The tolerability outcomes included the proportions of patients who withdrew from treatment for any reason and who experienced at least one adverse event (AE). Effect sizes were estimated by network meta-analyses within a frequentist framework.
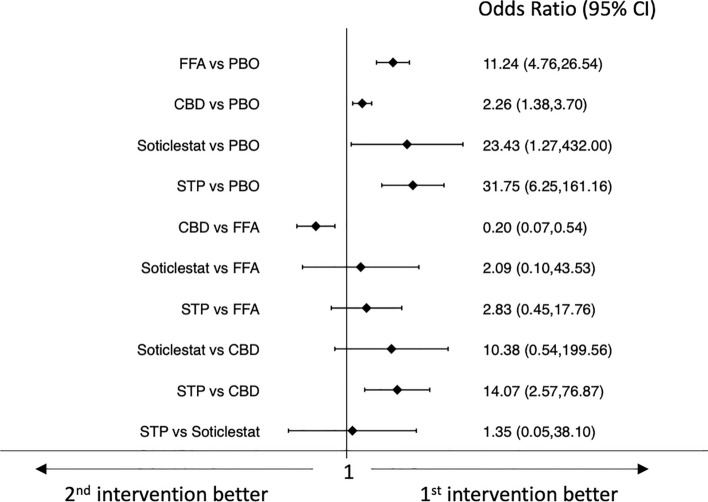
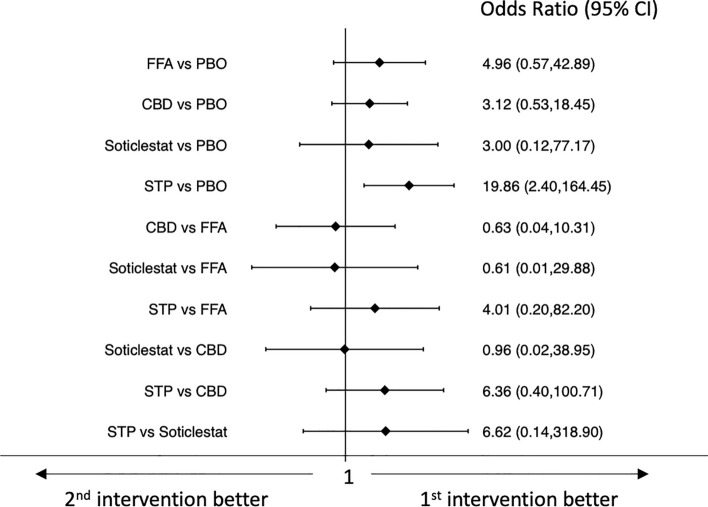
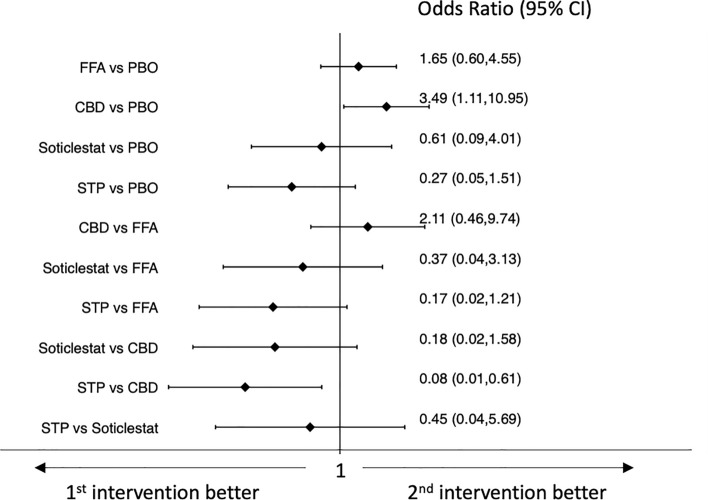
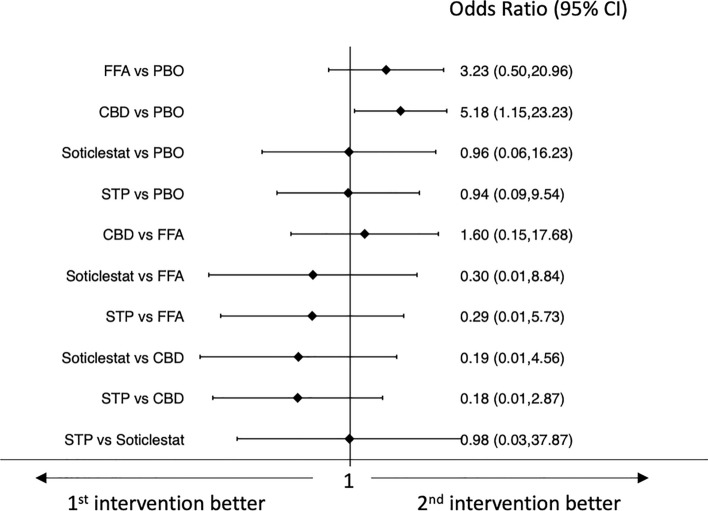
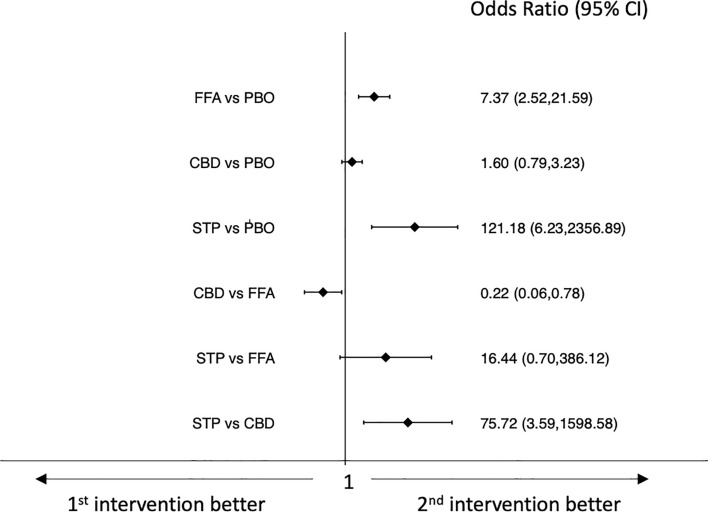
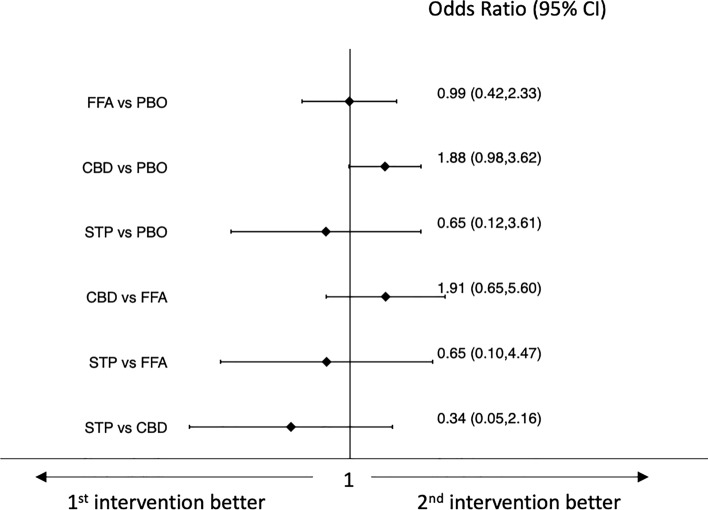
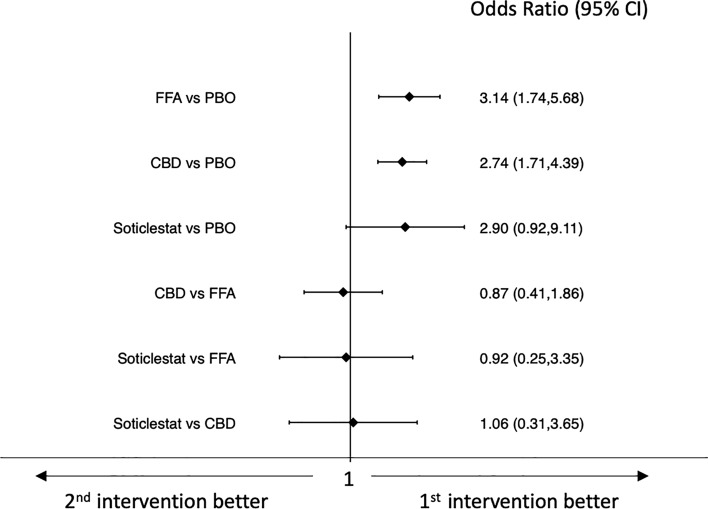
Results: Eight placebo-controlled trials were included, and the active add-on treatments were stiripentol (n = 2), pharmaceutical-grade cannabidiol (n = 3), fenfluramine hydrochloride (n = 2), and soticlestat (n = 1). The studies recruited 680 participants, of whom 409 were randomized to active treatments (stiripentol = 33, pharmaceutical-grade cannabidiol = 228, fenfluramine hydrochloride = 122, and soticlestat = 26) and 271 to placebo. Pharmaceutical-grade cannabidiol was associated with a lower rate of seizure response than fenfluramine hydrochloride (odds ratio [OR] 0.20, 95% confidence interval [CI] 0.07-0.54), and stiripentol was associated with a higher seizure response rate than pharmaceutical-grade cannabidiol (OR 14.07, 95% CI 2.57-76.87). No statistically significant differences emerged across the different ASMs for the seizure freedom outcome. Stiripentol was associated with a lower probability of drug discontinuation for any reason than pharmaceutical-grade cannabidiol (OR 0.45, 95% CI 0.04-5.69), and pharmaceutical-grade cannabidiol was associated with a lower proportion of participants experiencing any AE than fenfluramine hydrochloride (OR 0.22, 95% CI 0.06-0.78). Stiripentol had a higher risk of AE occurrence than pharmaceutical-grade cannabidiol (OR 75.72, 95% CI 3.59-1598.58). The study found high-quality evidence of efficacy and tolerability of the four ASMs in the treatment of convulsive seizures in DS.
Conclusions: There exists first-class evidence that documents the efficacy and tolerability of stiripentol, pharmaceutical-grade cannabidiol, fenfluramine hydrochloride, and soticlestat for the treatment of seizures associated with DS, and allows discussion about the expected outcomes regarding seizure frequency reduction and tolerability profiles.
© 2023. The Author(s).
Conflict of interest statement
Simona Lattanzi has received speaker’s or consultancy fees from Angelini Pharma, Eisai, GW Pharmaceuticals, and UCB Pharma, and has served on advisory boards for Angelini Pharma, Arvelle Therapeutics, BIAL, Eisai, GW Pharmaceuticals and Rapport Therapeutics outside the submitted work. Eugen Trinka received speaker’s honoraria from UCB Pharma, Biogen, Gerot-Lannach, Bial, Eisai, Takeda, Newbridge, Sunovion Pharmaceuticals Inc., LivaNova and Novartis; consultancy funds from UCB Pharma, Biogen, Gerot-Lannach, Bial, Eisai, Takeda, Newbridge, GW Pharmaceuticals, Sunovion Pharmaceuticals Inc., and Novartis outside the submitted work; and directorship funds from Neuroconsult GmbH. Furthermore, his institution received grants from Biogen, Red Bull, Merck, UCB Pharma, European Union, FWF Österreichischer Fond zur Wissenschaftsförderung, and Bundesministerium für Wissenschaft und Forschung. Emilio Russo has received speaker’s fees or funding from, and has participated in advisory boards for, Angelini, Arvelle Therapeutics, Eisai, Kolfarma, Pfizer, GW Pharmaceuticals, UCB Pharma, and Lundbeck outside the submitted work. Sara Matricardi has served on the advisory board for UCB Pharma, and has received consultancy fees from Eisai outside the submitted work. Stefano Meletti received research grant support from the Ministry of Health and the non-profit organization Foundation ‘Fondazione Cassa di Risparmio di Modena—FCRM’; and has received personal compensation as a scientific advisory board member for UCB and Eisai outside the submitted work. Pasquale Striano received fees and research grants from GW Pharmaceuticals, Zogenyx, Biomarin, and Kolfarma outside the submitted work. Cinzia Del Giovane, Payam Tabaee Damavandi, Mauro Silvestrini, and Francesco Brigo have no conflicts of interest to declare that are directly relevant to the contents of this study.
Figures