

The optimal healthy ranges of thyroid function defined by the risk of cardiovascular disease and mortality: systematic review and individual participant data meta-analysis
- PMID: 37696273
- PMCID: PMC10866328
- DOI: 10.1016/S2213-8587(23)00227-9
The optimal healthy ranges of thyroid function defined by the risk of cardiovascular disease and mortality: systematic review and individual participant data meta-analysis
Abstract
Background: Reference intervals of thyroid-stimulating hormone (TSH) and free thyroxine (FT4) are statistically defined by the 2·5-97·5th percentiles, without accounting for potential risk of clinical outcomes. We aimed to define the optimal healthy ranges of TSH and FT4 based on the risk of cardiovascular disease and mortality.
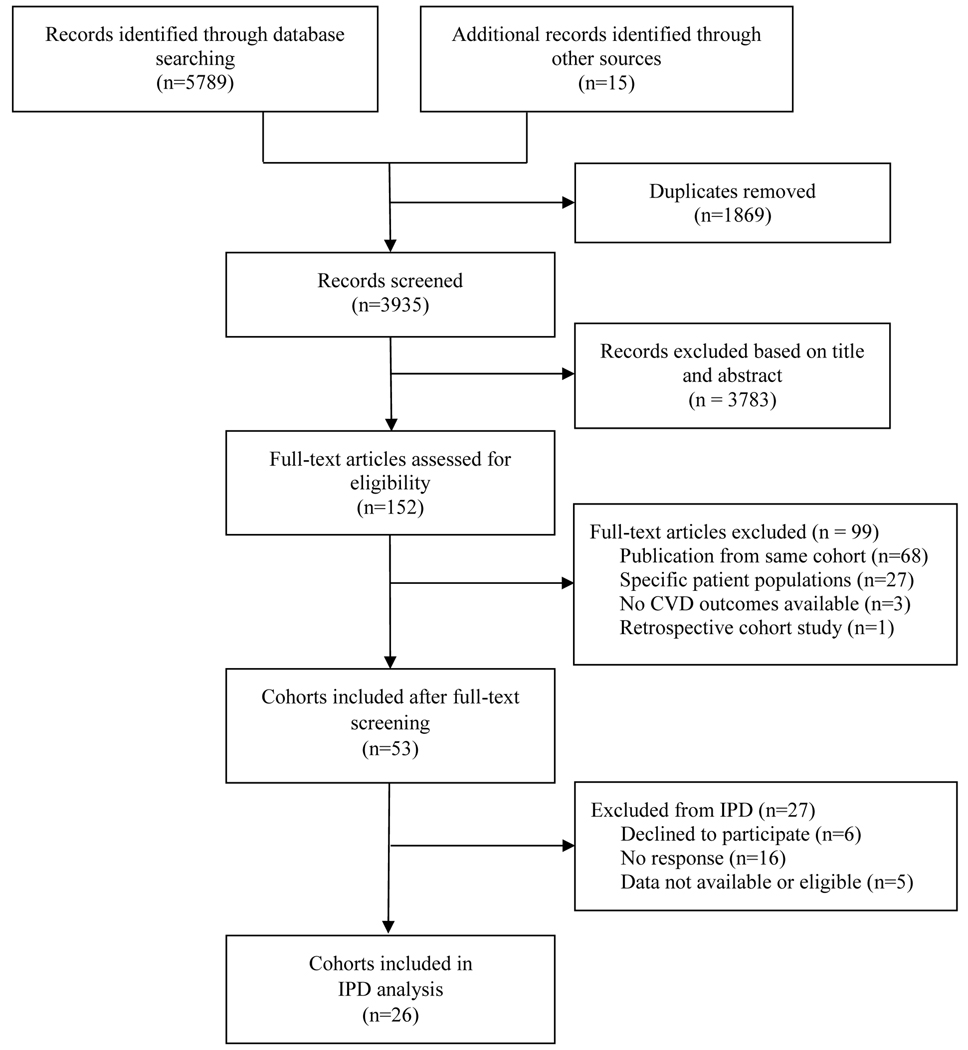
Methods: This systematic review and individual participant data (IPD) meta-analysis identified eligible prospective cohorts through the Thyroid Studies Collaboration, supplemented with a systematic search via Embase, MEDLINE (Ovid), Web of science, the Cochrane Central Register of Controlled Trials, and Google Scholar from Jan 1, 2011, to Feb 12, 2017 with an updated search to Oct 13, 2022 (cohorts found in the second search were not included in the IPD). We included cohorts that collected TSH or FT4, and cardiovascular outcomes or mortality for adults (aged ≥18 years). We excluded cohorts that included solely pregnant women, individuals with overt thyroid diseases, and individuals with cardiovascular disease. We contacted the study investigators of eligible cohorts to provide IPD on demographics, TSH, FT4, thyroid peroxidase antibodies, history of cardiovascular disease and risk factors, medication use, cardiovascular disease events, cardiovascular disease mortality, and all-cause mortality. The primary outcome was a composite outcome including cardiovascular disease events (coronary heart disease, stroke, and heart failure) and all-cause mortality. Secondary outcomes were the separate assessment of cardiovascular disease events, all-cause mortality, and cardiovascular disease mortality. We performed one-step (cohort-stratified Cox models) and two-step (random-effects models) meta-analyses adjusting for age, sex, smoking, systolic blood pressure, diabetes, and total cholesterol. The study was registered with PROSPERO, CRD42017057576.
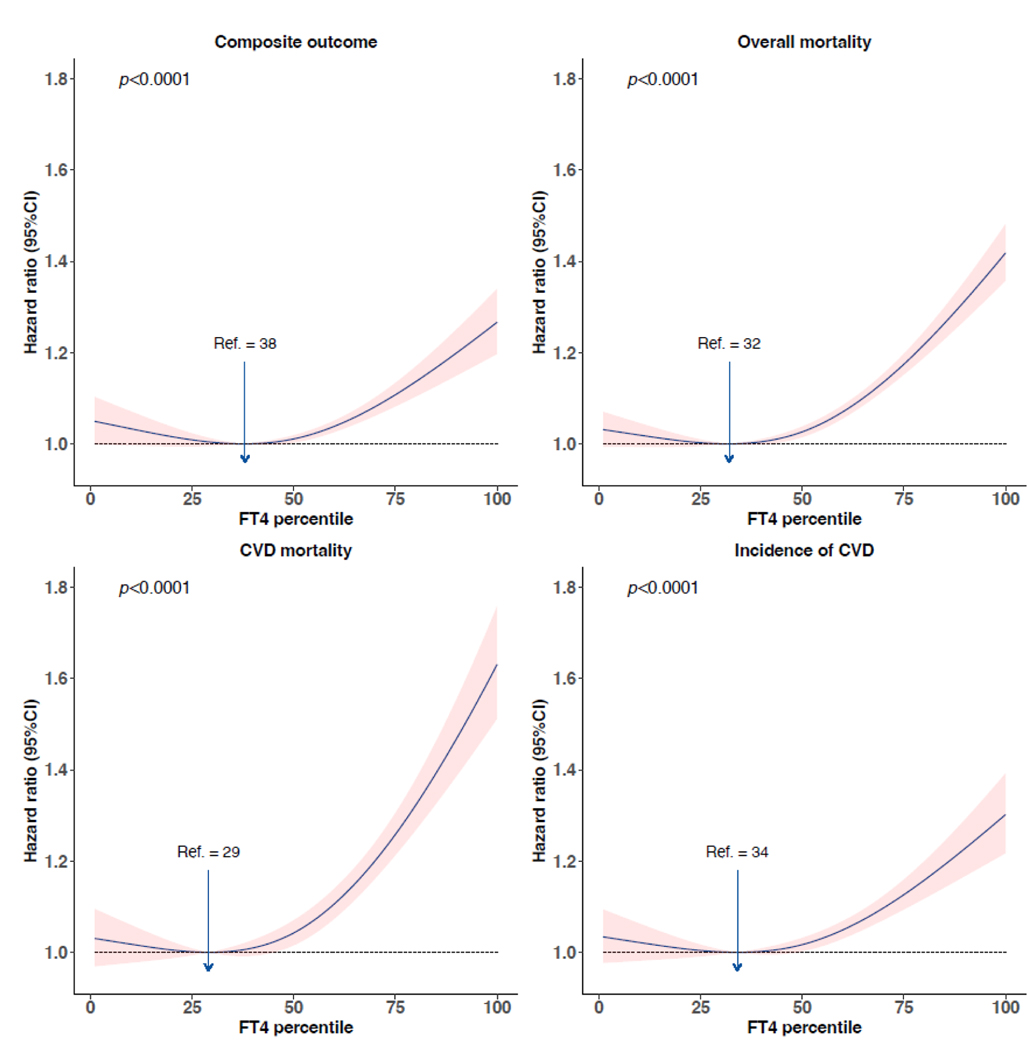
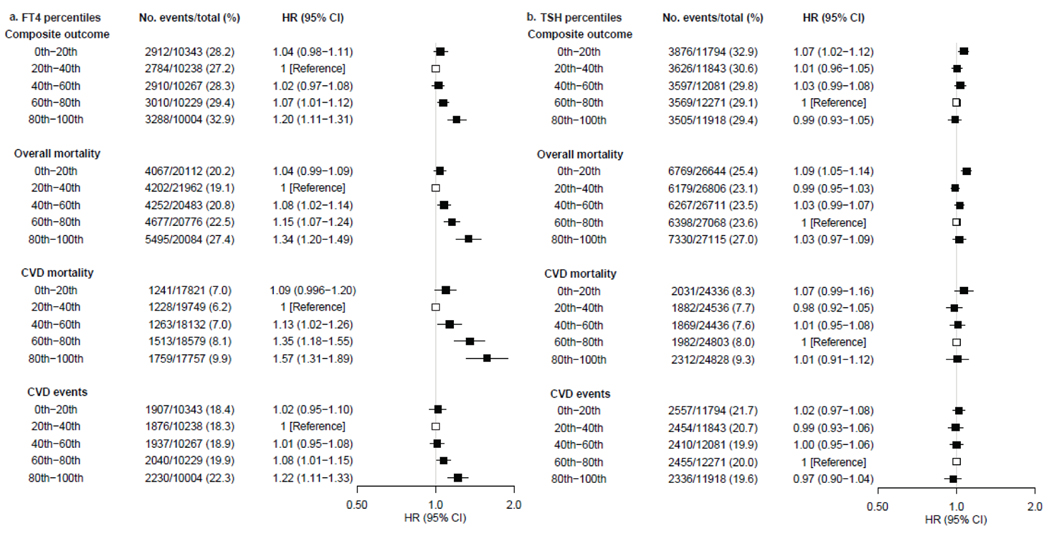
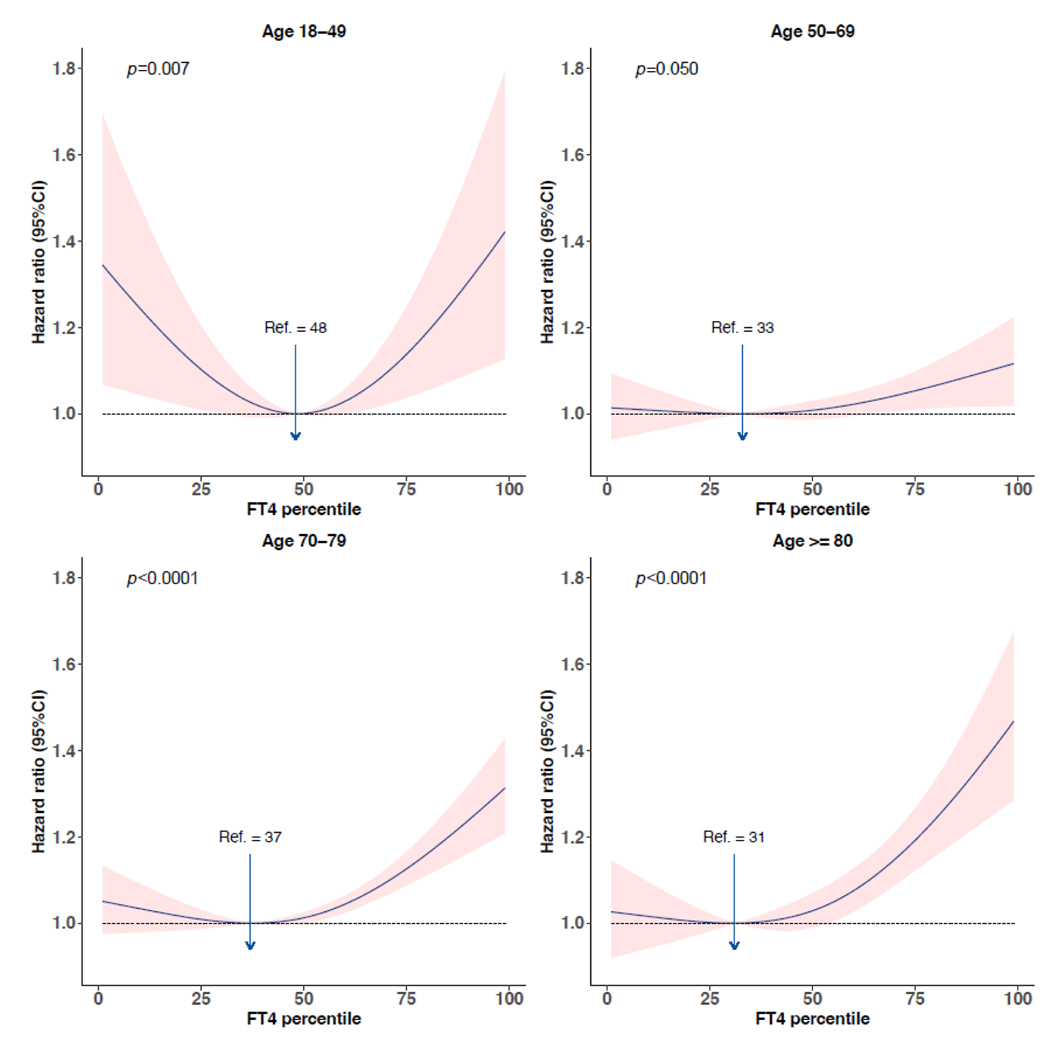
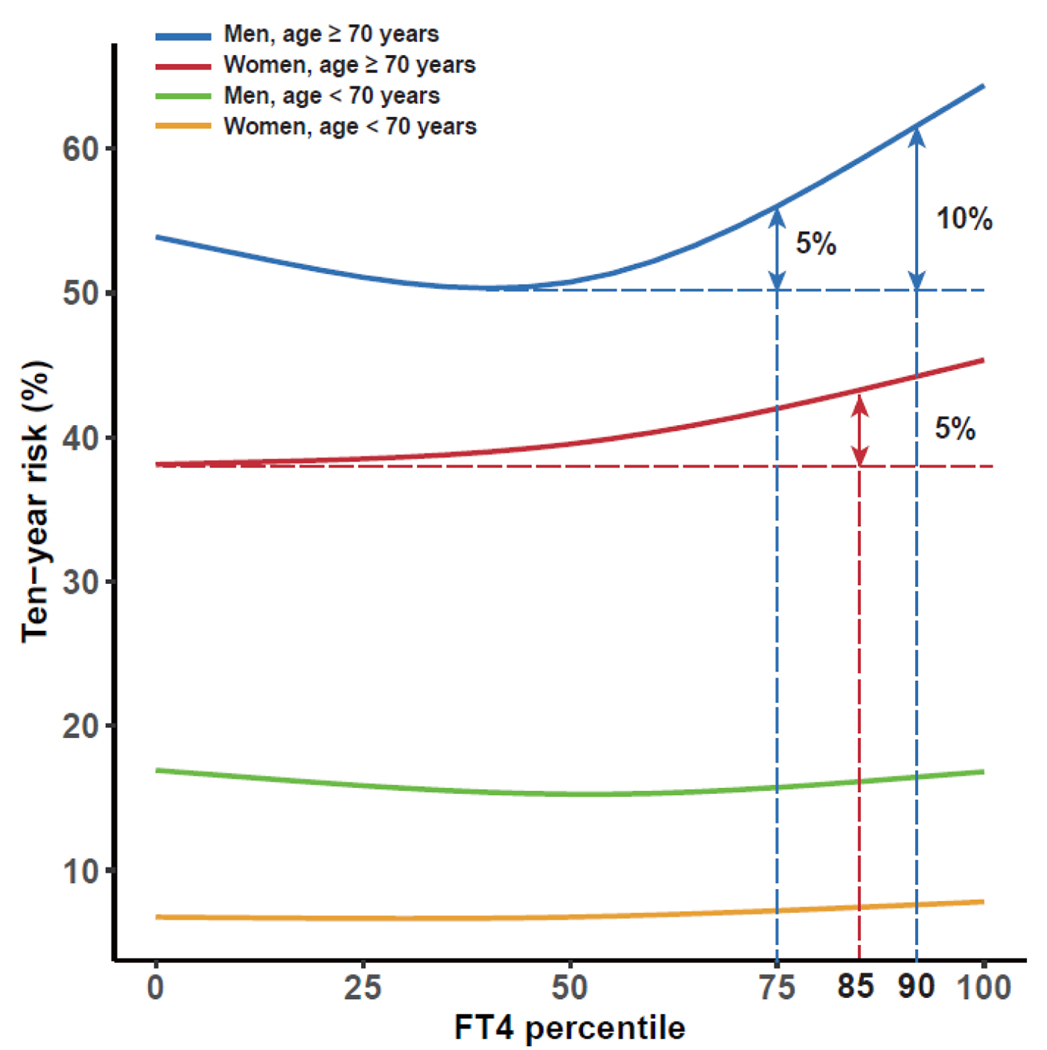
Findings: We identified 3935 studies, of which 53 cohorts fulfilled the inclusion criteria and 26 cohorts agreed to participate. We included IPD on 134 346 participants with a median age of 59 years (range 18-106) at baseline. There was a J-shaped association of FT4 with the composite outcome and secondary outcomes, with the 20th (median 13·5 pmol/L [IQR 11·2-13·9]) to 40th percentiles (median 14·8 pmol/L [12·3-15·0]) conveying the lowest risk. Compared with the 20-40th percentiles, the age-adjusted and sex-adjusted hazard ratio (HR) for FT4 in the 80-100th percentiles was 1·20 (95% CI 1·11-1·31) for the composite outcome, 1·34 (1·20-1·49) for all-cause mortality, 1·57 (1·31-1·89) for cardiovascular disease mortality, and 1·22 (1·11-1·33) for cardiovascular disease events. In individuals aged 70 years and older, the 10-year absolute risk of composite outcome increased over 5% for women with FT4 greater than the 85th percentile (median 17·6 pmol/L [IQR 15·0-18·3]), and men with FT4 greater than the 75th percentile (16·7 pmol/L [14·0-17·4]). Non-linear associations were identified for TSH, with the 60th (median 1·90 mIU/L [IQR 1·68-2·25]) to 80th percentiles (2·90 mIU/L [2·41-3·32]) associated with the lowest risk of cardiovascular disease and mortality. Compared with the 60-80th percentiles, the age-adjusted and sex-adjusted HR of TSH in the 0-20th percentiles was 1·07 (95% CI 1·02-1·12) for the composite outcome, 1·09 (1·05-1·14) for all-cause mortality, and 1·07 (0·99-1·16) for cardiovascular disease mortality.
Interpretation: There was a J-shaped association of FT4 with cardiovascular disease and mortality. Low concentrations of TSH were associated with a higher risk of all-cause mortality and cardiovascular disease mortality. The 20-40th percentiles of FT4 and the 60-80th percentiles of TSH could represent the optimal healthy ranges of thyroid function based on the risk of cardiovascular disease and mortality, with more than 5% increase of 10-year composite risk identified for FT4 greater than the 85th percentile in women and men older than 70 years. We propose a feasible approach to establish the optimal healthy ranges of thyroid function, allowing for better identification of individuals with a higher risk of thyroid-related outcomes.
Funding: None.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests TIMK reports personal fees from IBSA, Meck, Berlin-Chemie, and Quidel; is an unpaid co-chair of the American Thyroid Association guidelines on thyroid and pregnancy. BBY reports grants from National Health and Medical Research Council, Fremantle Hospital Medical Research Foundation, and Ada Bartholomew Medical Research Trust. NR reports a grant from the Swiss National Science Foundation. SR reports a grant for an investigator-initiated trial by Merck; manufacturer of levothyroxine and speaker fees from Merck, Abbott Pharmaceuticals, IBSA (makers of levothyroxine). JWJ reports research grants from or was a speaker (with or without lecture fees) at (Continuing Medical Education accredited) meetings sponsored or supported by Abbott, Amarin, Amgen, Athera, Biotronik, Boston Scientific, Dalcor, Daiichi Sankyo, Edwards Lifesciences, GE Healthcare, Johnson and Johnson, Lilly, Medtronic, Merck-Schering-Plough, Novartis, Novo Nordisk, Pfizer, Roche, Sanofi Aventis, the Netherlands Heart Foundation, CardioVascular Research the Netherlands, the Netherlands Heart Institute, and the European Community Framework KP7 Programme. DCB reports research grants from the National institutes of Health. DF reports a research grant from DFG SFB TR 296 LOCOTACT. RGJW reports a research grant from the Novo Nordisk Foundation Challenge Programme (NNF17OC0027812). All other authors declare no competing interests.
Figures
Comment in
-
Is it time to re-assess the development of thyroid function reference ranges?Lancet Diabetes Endocrinol. 2023 Oct;11(10):711-712. doi: 10.1016/S2213-8587(23)00257-7. Epub 2023 Sep 8. Lancet Diabetes Endocrinol. 2023. PMID: 37696274 No abstract available.
References
-
- Ozarda Y, Sikaris K, Streichert T, Macri J, intervals ICoR, Decision L. Distinguishing reference intervals and clinical decision limits - A review by the IFCC Committee on Reference Intervals and Decision Limits. Crit Rev Clin Lab Sci 2018; 55(6): 420–31. - PubMed
-
- Willett WC, Dietz WH, Colditz GA. Guidelines for healthy weight. N Engl J Med 1999; 341(6): 427–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC085080/HL/NHLBI NIH HHS/United States
- R01 AG027012/AG/NIA NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- K24 AG042765/AG/NIA NIH HHS/United States
- U01 AG042145/AG/NIA NIH HHS/United States
- R01 NR012459/NR/NINR NIH HHS/United States
- R01 AG028050/AG/NIA NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- U01 AG042143/AG/NIA NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- Z99 AG999999/ImNIH/Intramural NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- UL1 TR002369/TR/NCATS NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- R01 AG066671/AG/NIA NIH HHS/United States
- U01 AG042124/AG/NIA NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- U01 AG042168/AG/NIA NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- 75N92021D00006/HL/NHLBI NIH HHS/United States
- R01 AG032317/AG/NIA NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- MC_UU_00006/1/MRC_/Medical Research Council/United Kingdom
- N01 HC085081/HL/NHLBI NIH HHS/United States
- U01 AG042139/AG/NIA NIH HHS/United States
