

Leveraging Electronic Health Records to Construct a Phenotype for Hypertension Surveillance in the United States
- PMID: 37696605
- PMCID: PMC10898654
- DOI: 10.1093/ajh/hpad081
Leveraging Electronic Health Records to Construct a Phenotype for Hypertension Surveillance in the United States
Abstract
Background: Hypertension is an important risk factor for cardiovascular diseases. Electronic health records (EHRs) may augment chronic disease surveillance. We aimed to develop an electronic phenotype (e-phenotype) for hypertension surveillance.
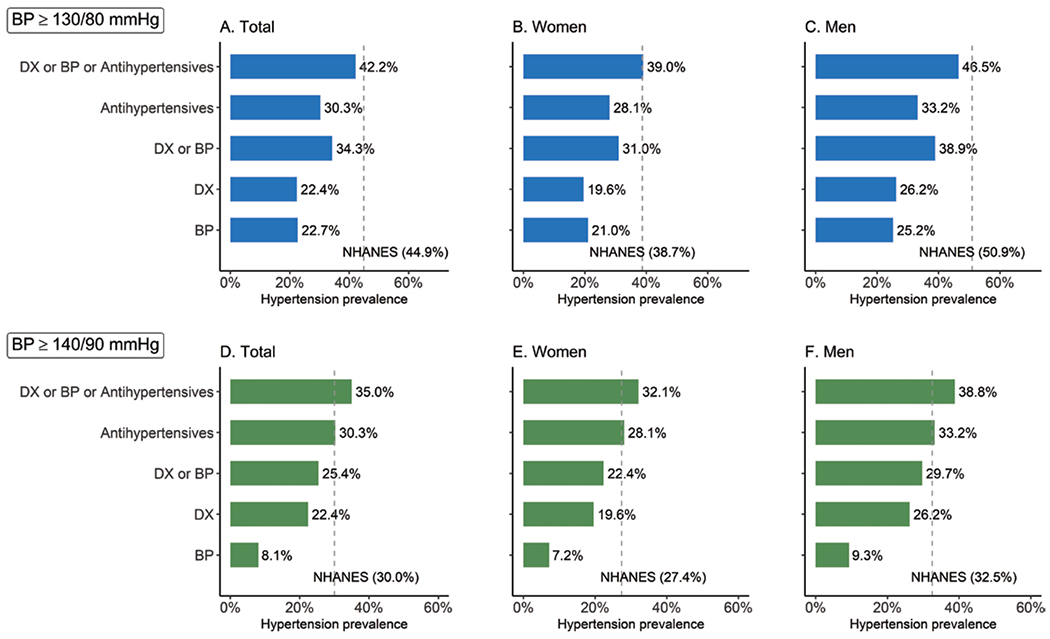
Methods: We included 11,031,368 eligible adults from the 2019 IQVIA Ambulatory Electronic Medical Records-US (AEMR-US) dataset. We identified hypertension using three criteria, alone or in combination: diagnosis codes, blood pressure (BP) measurements, and antihypertensive medications. We compared AEMR-US estimates of hypertension prevalence and control against those from the National Health and Nutrition Examination Survey (NHANES) 2017-18, which defined hypertension as BP ≥130/80 mm Hg or ≥1 antihypertensive medication.
Results: The study population had a mean (SD) age of 52.3 (6.7) years, and 56.7% were women. The selected three-criteria e-phenotype (≥1 diagnosis code, ≥2 BP measurements of ≥130/80 mm Hg, or ≥1 antihypertensive medication) yielded similar trends in hypertension prevalence as NHANES: 42.2% (AEMR-US) vs. 44.9% (NHANES) overall, 39.0% vs. 38.7% among women, and 46.5% vs. 50.9% among men. The pattern of age-related increase in hypertension prevalence was similar between AEMR-US and NHANES. The prevalence of hypertension control in AEMR-US was 31.5% using the three-criteria e-phenotype, which was higher than NHANES (14.5%).
Conclusions: Using an EHR dataset of 11 million adults, we constructed a hypertension e-phenotype using three criteria, which can be used for surveillance of hypertension prevalence and control.
Keywords: blood pressure; chronic disease; electronic health record; hypertension; phenotype; surveillance.
© Published by Oxford University Press on behalf of American Journal of Hypertension Ltd 2023.
Conflict of interest statement
Disclosure
The authors have no conflict of interest to declare.
Figures


Similar articles
-
US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008.JAMA. 2010 May 26;303(20):2043-50. doi: 10.1001/jama.2010.650. JAMA. 2010. PMID: 20501926
-
Development of a Hypertension Electronic Phenotype for Chronic Disease Surveillance in Electronic Health Records: Key Analytic Decisions and Their Effects.Prev Chronic Dis. 2023 Sep 14;20:E80. doi: 10.5888/pcd20.230026. Prev Chronic Dis. 2023. PMID: 37708339 Free PMC article.
-
Trends in Blood Pressure Control Among US Adults With Hypertension, 1999-2000 to 2017-2018.JAMA. 2020 Sep 22;324(12):1190-1200. doi: 10.1001/jama.2020.14545. JAMA. 2020. PMID: 32902588 Free PMC article.
-
National surveillance definitions for hypertension prevalence and control among adults.Circ Cardiovasc Qual Outcomes. 2012 May;5(3):343-51. doi: 10.1161/CIRCOUTCOMES.111.963439. Epub 2012 May 1. Circ Cardiovasc Qual Outcomes. 2012. PMID: 22550130 Free PMC article. Review.
-
What is the prevalence of resistant hypertension in the United States?Curr Opin Cardiol. 2012 Jul;27(4):386-91. doi: 10.1097/HCO.0b013e328353ad6e. Curr Opin Cardiol. 2012. PMID: 22596184 Review.
Cited by
-
Rurality, Cardiovascular Risk Factors, and Early Cardiovascular Disease among Childhood, Adolescent, and Young Adult Cancer Survivors.Res Sq [Preprint]. 2024 Apr 1:rs.3.rs-4139837. doi: 10.21203/rs.3.rs-4139837/v1. Res Sq. 2024. Update in: J Adolesc Young Adult Oncol. 2025 Mar 25. doi: 10.1089/jayao.2024.0151. PMID: 38645102 Free PMC article. Updated. Preprint.
-
Hypertension and Polycystic Ovary Syndrome Among Women in a Nationwide Electronic Health Records Dataset in the United States.Matern Child Health J. 2025 Sep 1. doi: 10.1007/s10995-025-04155-x. Online ahead of print. Matern Child Health J. 2025. PMID: 40889056
-
State-Level Hypertension Prevalence and Control Among Adults in the U.S.Am J Prev Med. 2024 Jan;66(1):46-54. doi: 10.1016/j.amepre.2023.09.010. Epub 2023 Oct 25. Am J Prev Med. 2024. PMID: 37877903 Free PMC article.
-
Hypertension in Pregnancy: Current Challenges and Future Opportunities for Surveillance and Research.J Womens Health (Larchmt). 2024 May;33(5):553-562. doi: 10.1089/jwh.2023.1072. Epub 2024 Mar 26. J Womens Health (Larchmt). 2024. PMID: 38529887 Free PMC article.
-
Hypertension Prevalence and Control Among U.S. Women of Reproductive Age.Am J Prev Med. 2024 Mar;66(3):492-502. doi: 10.1016/j.amepre.2023.10.016. Epub 2023 Oct 24. Am J Prev Med. 2024. PMID: 37884175 Free PMC article.
References
-
- Hypertension Cascade: Hypertension Prevalence. Treatment and Control Estimates Among US Adults Aged 18 Years and Older Applying the Criteria From the American College of Cardiology and American Heart Association’s 2017 Hypertension Guideline—NHANES 2015–2018. US Department of Health and Human Services; 2021, Centers for Disease Control and Prevention (CDC): Atlanta, GA, 2021.
-
- Multiple Cause of Death, 1999–2020 Request. https://wonder.cdc.gov/mcd-icd10.html. Accessed 20 July 2022.
-
- Farley TA, Dalal MA, Mostashari F, Frieden TR, Frieden TR. Deaths preventable in the U.S. by improvements in use of clinical preventive services. Am J Prev Med 2010; 38(6):600–609. - PubMed
-
- Rahimi K, Bidel Z, Nazarzadeh M, Copland E, Canoy D, Ramakrishnan R, Pinho-Gomes A-C, Woodward M, Adler A, Agodoa L, Algra A, Asselbergs FW, Beckett NS, Berge E, Black H, Brouwers FPJ, Brown M, Bulpitt CJ, Byington RP, Cushman WC, Cutler J, Devereaux RB, Dwyer J, Estacio R, Fagard R, Fox K, Fukui T, Gupta AK, Holman RR, Imai Y, Ishii M, Julius S, Kanno Y, Kjeldsen SE, Kostis J, Kuramoto K, Lanke J, Lewis E, Lewis JB, Lievre M, Lindholm LH, Lueders S, MacMahon S, Mancia G, Matsuzaki M, Mehlum MH, Nissen S, Ogawa H, Ogihara T, Ohkubo T, Palmer CR, Patel A, Pfeffer MA, Pitt B, Poulter NR, Rakugi H, Reboldi G, Reid C, Remuzzi G, Ruggenenti P, Saruta T, Schrader J, Schrier R, Sever P, Sleight P, Staessen JA, Suzuki H, Thijs L, Ueshima K, Umemoto S, van Gilst WH, Verdecchia P, Wachtell K, Whelton P, Wing L, Yui Y, Yusuf S, Zanchetti A, Zhang Z-Y, Anderson C, Baigent C, Brenner BM, Collins R, de Zeeuw D, Lubsen J, Malacco E, Neal B, Perkovic V, Rodgers A, Rothwell P, Salimi-Khorshidi G, Sundström J, Turnbull F, Viberti G, Wang J, Chalmers J, Teo KK, Pepine CJ, Davis BR. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis. Lancet 2021; 397(10285):1625–1636. - PMC - PubMed
-
- Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General. The Surgeon General’s Call to Action to Control Hypertension. U.S. Department of Health and Human Services: Washington, DC, 2020.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
