

Zanubrutinib: past, present, and future
- PMID: 37696810
- PMCID: PMC10495438
- DOI: 10.1038/s41408-023-00902-x
Zanubrutinib: past, present, and future
Erratum in
-
Correction: Zanubrutinib: past, present, and future.Blood Cancer J. 2023 Oct 2;13(1):154. doi: 10.1038/s41408-023-00926-3. Blood Cancer J. 2023. PMID: 37783709 Free PMC article. No abstract available.
Abstract
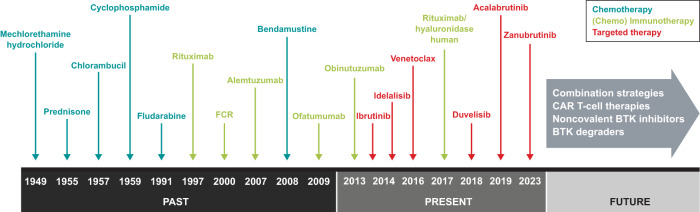
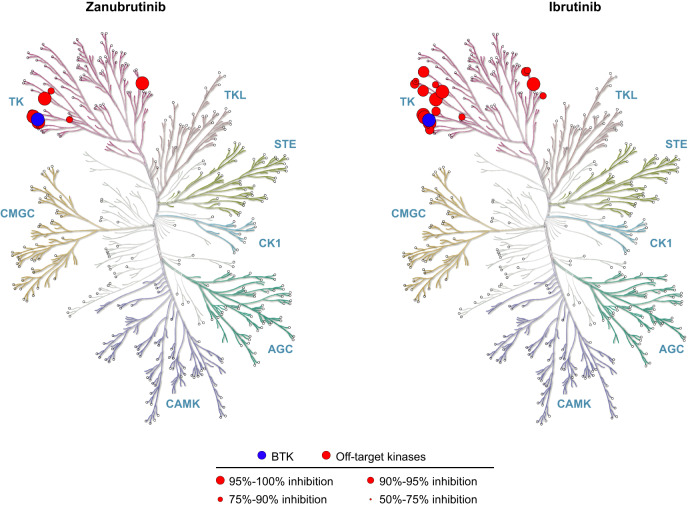
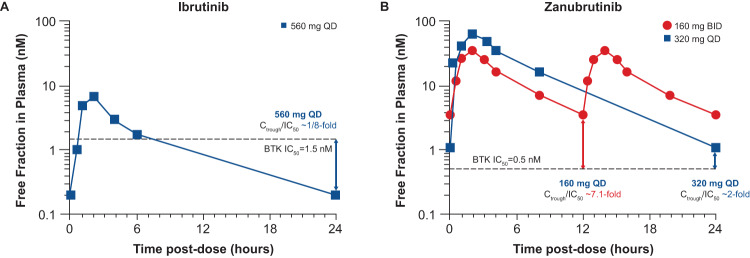
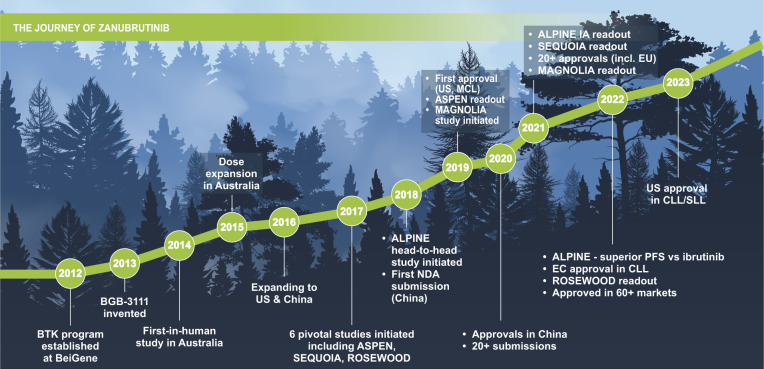
In recent years, Bruton tyrosine kinase (BTK) inhibitors have provided significant advances in the treatment of patients with B-cell malignancies. Ibrutinib was the first BTK inhibitor to be approved, and it changed the standard-of-care treatment for diseases such as chronic lymphocytic leukemia, mantle cell lymphoma, marginal zone lymphoma, and Waldenström macroglobulinemia, improving efficacy outcomes and safety compared to chemotherapy. In this article, we review the development of zanubrutinib, a next-generation BTK inhibitor, from molecular design to patient-related outcomes. We start this journey by providing insights into the discovery of BTK and the physiologic, genetic, and molecular characterization of patients lacking this kinase, together with the brief treatment landscape in the era of chemo-immunotherapies. Zanubrutinib was originally developed by applying a structure-activity strategy to enhance the specificity as well as enzymatic and pharmacokinetic properties. Preclinical studies confirmed greater specificity and better bioavailability of zanubrutinib compared with that of ibrutinib, which supported the initiation of clinical trials in humans. Preliminary clinical results indicated activity in B-cell malignancies together with an improved safety profile, in line with less off-target effects described in the preclinical studies. The clinical program of zanubrutinib has since expanded significantly, with ongoing studies in a wide range of hemato-oncological diseases and in combination with many other therapies. Zanubrutinib currently is approved for various B-cell malignancies in multiple countries. This story highlights the importance of multidisciplinary collaborative research, from bench to bedside, and provides an example of how the commitment to finding improved treatment options should always run parallel to patient care.
© 2023. Springer Nature Limited.
Conflict of interest statement
JM reports consulting fees from ADC Therapeutics, Alexion, Bayer, BeiGene, BMS, Debiopharm, Epizyme, Fosun Kite, Genmab, Gilead/Kite Pharma, Innovent, Janssen, Juno/Celgene, Karyopharm, Kyowa, MorphoSys/Incyte, Novartis, Pfizer, Pharmacyclics/AbbVie, Seagen, and Servier; research funding from Bayer, Celgene, Genentech, Gilead/Kite Pharma, Incyte, Janssen, Merck, Millennium, Pharmacyclics, Portola, and Seagen; honoraria from Curio, Kyowa, OncView, Physicians’ Education Resource, Seagen, and Targeted Oncology; and speakers bureau for Acrotech/Aurobindo, AstraZeneca, Bayer, BeiGene, Celgene/BMS, Genentech/Roche, Gilead/Kite Pharma, Pharmacyclics/Janssen, Kyowa, Seagen, and Verastem. JFS reports research funding from AbbVie, BMS, and Roche; and advisory board/honoraria from AbbVie, AstraZeneca, BeiGene, BMS, Genentech, Genor Bio, Gilead, Janssen, Roche, Sunesis, and TG Therapeutics. CST received research support from Janssen and AbbVie; received honoraria from BeiGene, AbbVie, and Janssen; and received other remuneration from BeiGene. SO reports funding from BeiGene paid to Monash University, with regards to the submitted work; receiving honoraria and participating on an advisory board for BeiGene, outside the submitted work.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
