

Treatment of older adults with FLT3-mutated AML: Emerging paradigms and the role of frontline FLT3 inhibitors
- PMID: 37696819
- PMCID: PMC10495326
- DOI: 10.1038/s41408-023-00911-w
Treatment of older adults with FLT3-mutated AML: Emerging paradigms and the role of frontline FLT3 inhibitors
Abstract
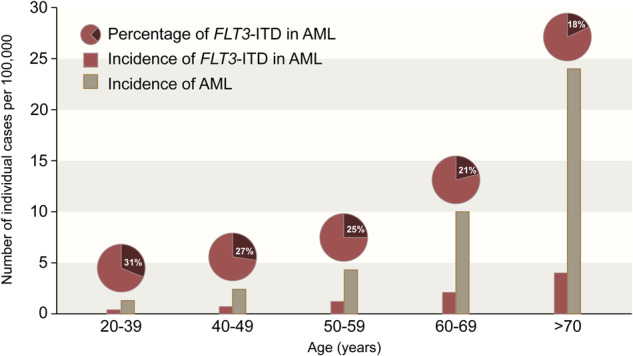
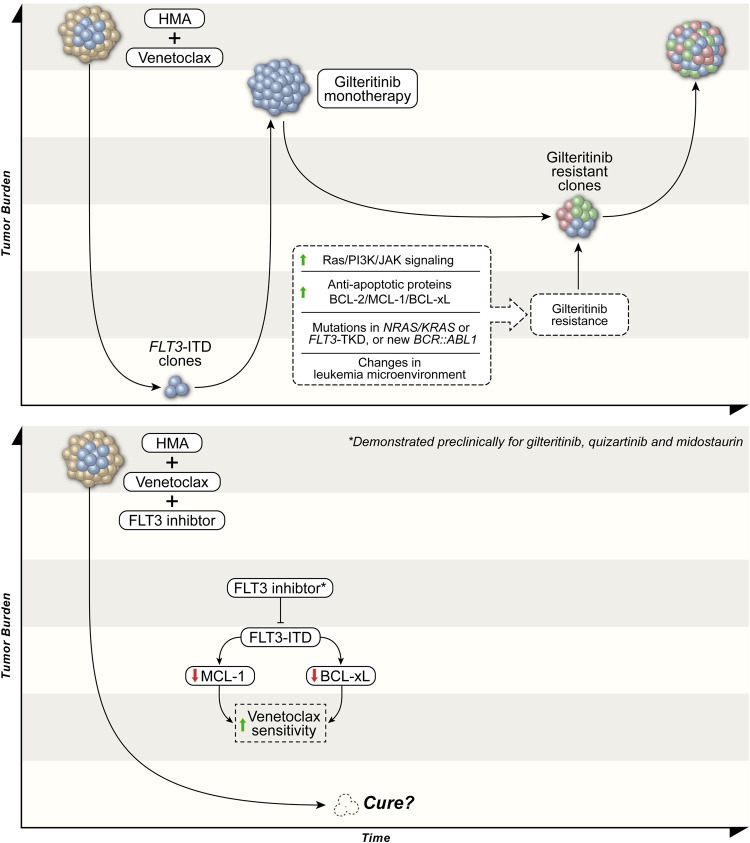
FLT3 is the most frequently mutated gene in acute myeloid leukemia (AML), with FLT3 internal tandem duplication (ITD) mutations being associated with a more aggressive clinical course. While two large, randomized clinical trials have shown a survival benefit with the frontline use of an oral FLT3 inhibitor (midostaurin or quizartinib) in patients with FLT3-mutated AML, the role of FLT3 inhibitors in older adults with newly diagnosed FLT3-mutated AML remains unclear. A definitive improvement in survival has not been observed in intensively treated patients over 60 years of age receiving frontline FLT3 inhibitors. Furthermore, many patients with FLT3-mutated AML are unsuitable for intensive chemotherapy due to age and/or comorbidities, and this population represents a particular unmet need. For these older patients who are unfit for intensive approaches, azacitidine + venetoclax is a new standard of care and is used by many clinicians irrespective of FLT3 mutation status. However, FLT3-ITD mutations confer resistance to venetoclax and are a well-established mechanism of relapse to lower-intensity venetoclax-based regimens, leading to short durations of remission and poor survival. Preclinical and clinical data suggest synergy between FLT3 inhibitors and venetoclax, providing rationale for their combination. Novel strategies to safely incorporate FLT3 inhibitors into the standard hypomethylating agent + venetoclax backbone are now being explored in this older, less fit population with newly diagnosed FLT3-mutated AML, with encouraging early results. Herein, we discuss the frontline use of FLT3 inhibitors in older adults with FLT3-mutated AML, including the potential role of FLT3 inhibitors in combination with intensive chemotherapy and as part of novel, lower-intensity doublet and triplet regimens in this older population.
© 2023. Springer Nature Limited.
Conflict of interest statement
NJS has served as consultant for Pfizer Inc., GSK, NKARTA, and Sanofi, reports receiving research grants from Takeda Oncology, Astellas Pharma Inc., Xencor, Stemline Therapeutics, and NextCure, and has received honoraria from Novartis, Amgen, Takeda Oncology, Astellas Pharma Inc., Sanofi, and BeiGene. FR has served as a consultant for AbbVie, reports receiving research grants from Astellas Pharma Inc. and Celgene/BMS, and has received honoraria from Astellas Pharma Inc. and Celgene/BMS. The other authors report no relevant conflicts of interest.
Figures
References
-
- Short NJ, Konopleva M, Kadia TM, Borthakur G, Ravandi F, DiNardo CD, et al. Advances in the treatment of acute myeloid leukemia: new drugs and new challenges. Cancer Discov. 2020;10:506–25.. - PubMed
-
- Dohner H, Wei AH, Lowenberg B. Towards precision medicine for AML. Nat Rev Clin Oncol. 2021;18:577–90.. - PubMed
-
- Tsai CH, Hou HA, Tang JL, Liu CY, Lin CC, Chou WC, et al. Genetic alterations and their clinical implications in older patients with acute myeloid leukemia. Leukemia. 2016;30:1485–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
