

Real-world evidence of ocrelizumab-treated relapsing multiple sclerosis cohort shows changes in progression independent of relapse activity mirroring phase 3 trials
- PMID: 37696848
- PMCID: PMC10495413
- DOI: 10.1038/s41598-023-40940-w
Real-world evidence of ocrelizumab-treated relapsing multiple sclerosis cohort shows changes in progression independent of relapse activity mirroring phase 3 trials
Abstract
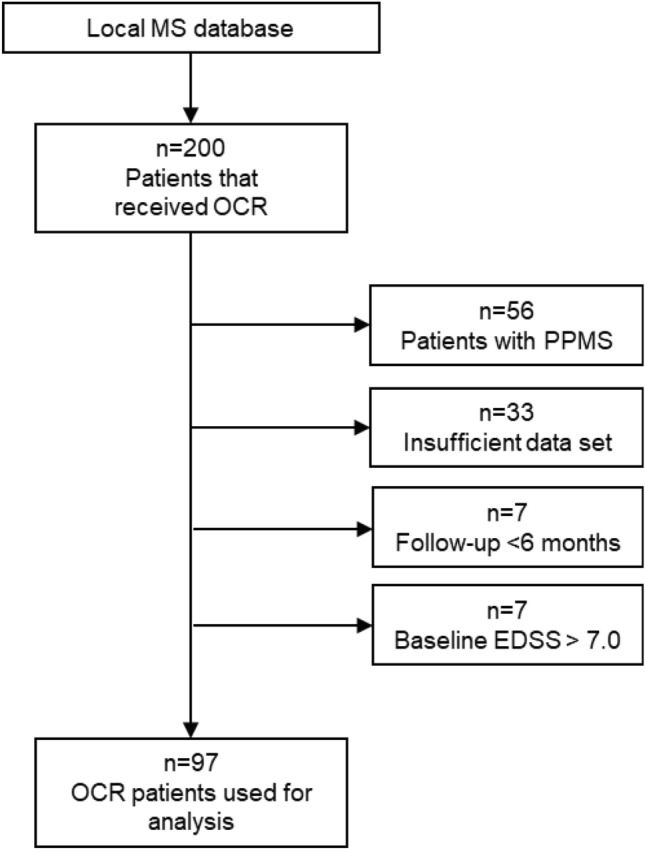
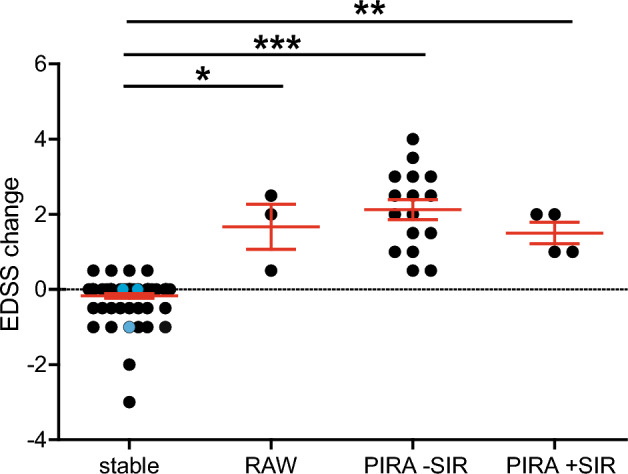
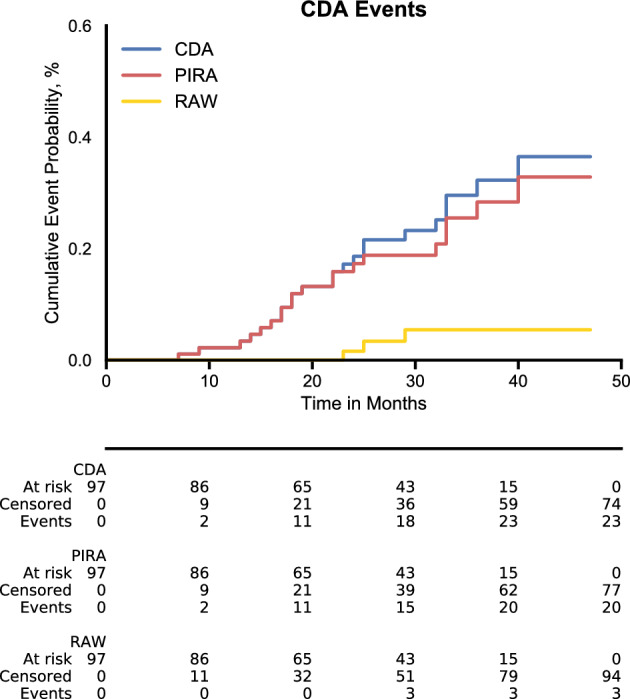
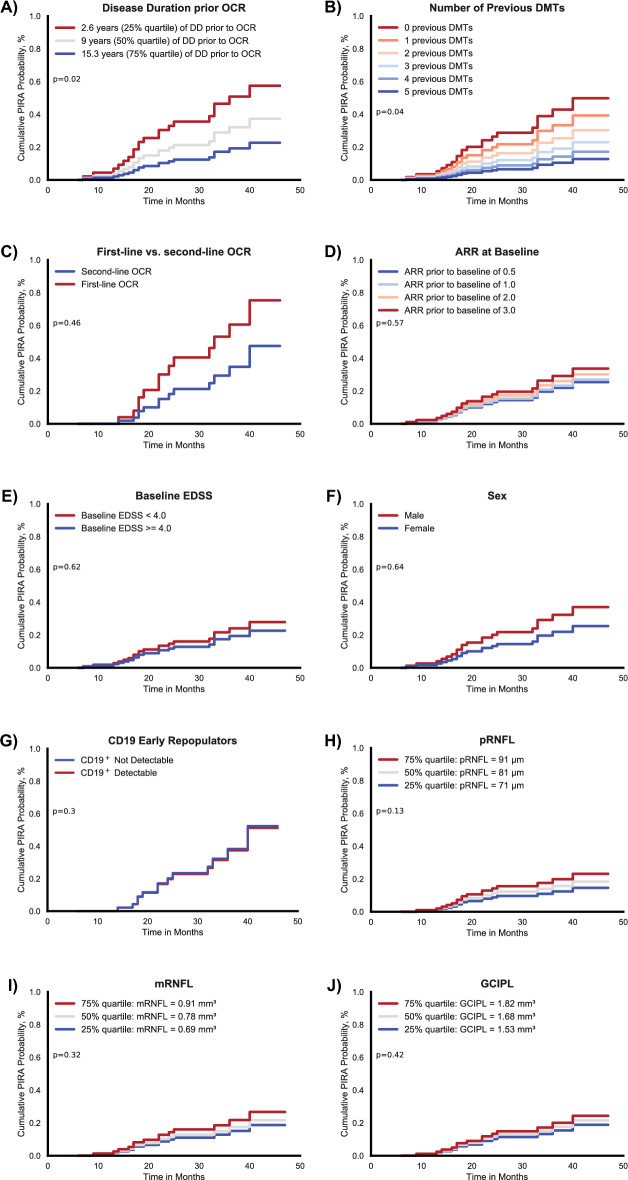
Ocrelizumab is a B cell-depleting drug widely used in relapsing-remitting multiple sclerosis (RRMS) and primary-progressive MS. In RRMS, it is becoming increasingly apparent that accumulation of disability not only manifests as relapse-associated worsening (RAW) but also as progression independent of relapse activity (PIRA) throughout the disease course. This study's objective was to investigate the role of PIRA in RRMS patients treated with ocrelizumab. We performed a single-center, retrospective, cross-sectional study of clinical data acquired at a German tertiary multiple sclerosis referral center from 2018 to 2022. All patients with RRMS treated with ocrelizumab for at least six months and complete datasets were analyzed. Confirmed disability accumulation (CDA) was defined as a ≥ 12-week confirmed increase from the previous expanded disability status scale (EDSS) score of ≥ 1.0 if the previous EDSS was ≤ 5.5 or a ≥ 0.5-point increase if the previous EDSS was > 5.5. PIRA was defined as CDA without relapse since the last EDSS measurement and at least for the preceding 12 weeks. RAW was defined as CDA in an interval of EDSS measurements with ≥ 1 relapses. Cox proportional hazard models were used to analyze the probability of developing PIRA depending on various factors, including disease duration, previous disease-modifying treatments (DMTs), and optical coherence tomography-assessed retinal degeneration parameters. 97 patients were included in the analysis. Mean follow-up time was 29 months (range 6 to 51 months). 23.5% developed CDA under ocrelizumab therapy (n = 23). Of those, the majority developed PIRA (87.0% of CDA, n = 20) rather than RAW (13.0% of CDA, n = 3). An exploratory investigation using Cox proportional hazards ratios revealed two possible factors associated with an increased probability of developing PIRA: a shorter disease duration prior to ocrelizumab (p = 0.02) and a lower number of previous DMTs prior to ocrelizumab (p = 0.04). Our data show that in ocrelizumab-treated RRMS patients, the main driver of disability accumulation is PIRA rather than RAW. Furthermore, these real-world data show remarkable consistency with data from phase 3 randomized controlled trials of ocrelizumab in RRMS, which may increase confidence in translating results from tightly controlled RCTs into the real-world clinical setting.
© 2023. Springer Nature Limited.
Conflict of interest statement
JI reports no conflicts of interest and funding by the Bundesinstitut für Risikobewertung (BfR), LM received honoraria from Biogen and Merck, as well as research funding from the Deutsche Multiple Sklerose Gesellschaft, MP received honoraria for lecturing from Argenx, Alexion, Novartis, Bayer Health Care, Sanofi-Aventis, Biogen and Merck; SS received no financial compensation or support from any organization or entity that may have an interest in the content of this manuscript; MW declares nor conflict of interest and nor funding received for the preparation of this report; OA has received, with approval of the Heinrich Heine University, advisor fees, honoraria, or travel reimbursements from Alexion, Almirall, Biogen, Horizon, MedImmune, Merck, Novartis, Roche, and Teva; research support from the German Science Foundation (DFG), the German Ministry of Education and Research (BMBF), Biogen, and Novartis. He is member of the European Reference Network—Eye Diseases (ERN-EYE) consortium and member of the German Neuromyelitis optica Study Group (NEMOS); SGM received honoraria for lecturing and travel expenses for attending meetings from Almirall, Amicus Therapeutics Germany, Bayer Health Care, Biogen, Celgene, Diamed, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Novo Nordisk, ONO Pharma, Roche, Sanofi-Aventis, Chugai Pharma, QuintilesIMS, and Teva. His research is funded by the German Ministry for Education and Research (BMBF), Bundesinstitut für Risikobewertung (BfR), Deutsche Forschungsgemeinschaft (DFG), Else Kröner Fresenius Foundation, Gemeinsamer Bundesausschuss (G-BA), German Academic Exchange Service, Hertie Foundation, Interdisciplinary Center for Clinical Studies (IZKF) Muenster, German Foundation Neurology and by Alexion, Almirall, Amicus Therapeutics Germany, Biogen, Diamed, Fresenius Medical Care, Genzyme, HERZ Burgdorf, Merck Serono, Novartis, ONO Pharma, Roche, and Teva; PA received research grants from BMS, Celgene, German Research Association, EFRE NRW, Ipsen, Merck, Merz, Novartis and speaker honoraria, travel support and recompensation for serving on advisory boards from Allergan, Abbvie, BMS, Celgene, Ipsen, Hexal, Janssen Cilag, Lilly, Merck, Merz, Novartis, Sanofi, TEVA.
Figures
References
-
- Kappos L, et al. Contribution of relapse-independent progression vs relapse-associated worsening to overall confirmed disability accumulation in typical relapsing multiple sclerosis in a pooled analysis of 2 randomized clinical trials. JAMA Neurol. 2020;77:1132–1140. doi: 10.1001/jamaneurol.2020.1568. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
