

High risk clear cell renal cell carcinoma microenvironments contain protumour immunophenotypes lacking specific immune checkpoints
- PMID: 37696903
- PMCID: PMC10495390
- DOI: 10.1038/s41698-023-00441-5
High risk clear cell renal cell carcinoma microenvironments contain protumour immunophenotypes lacking specific immune checkpoints
Abstract
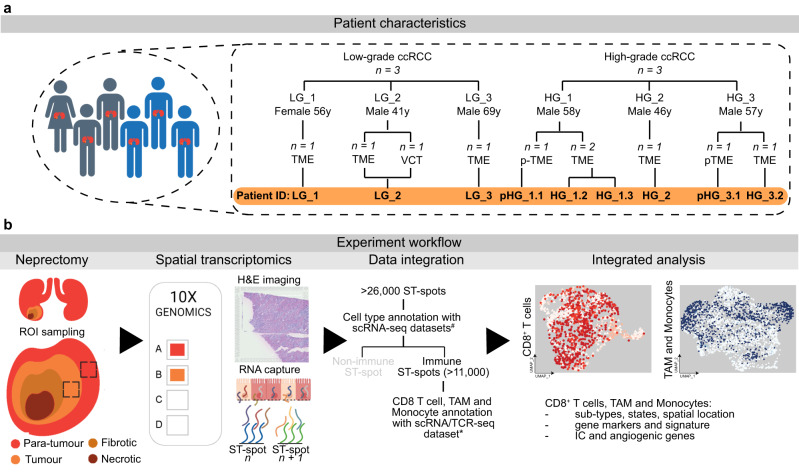
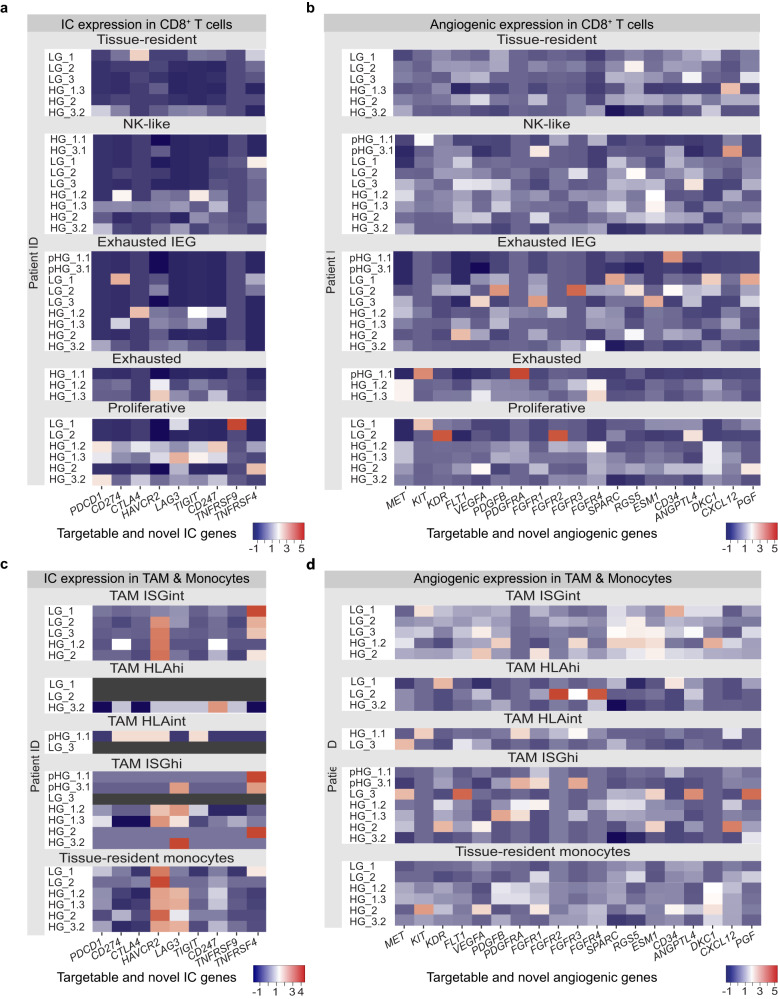
Perioperative immune checkpoint inhibitor (ICI) trials for intermediate high-risk clear cell renal cell carcinoma (ccRCC) have failed to consistently demonstrate improved patient outcomes. These unsuccessful ICI trials suggest that the tumour infiltrating immunophenotypes, termed here as the immune cell types, states and their spatial location within the tumour microenvironment (TME), were unfavourable for ICI treatment. Defining the tumour infiltrating immune cells may assist with the identification of predictive immunophenotypes within the TME that are favourable for ICI treatment. To define the immunophenotypes within the ccRCC TME, fresh para-tumour (pTME, n = 2), low-grade (LG, n = 4, G1-G2) and high-grade (HG, n = 4, G3-G4) tissue samples from six patients with ccRCC presenting at a tertiary referral hospital underwent spatial transcriptomics sequencing (ST-seq). Within the generated ST-seq datasets, immune cell types and states, termed here as exhausted/pro-tumour state or non-exhausted/anti-tumour state, were identified using multiple publicly available single-cell RNA and T-cell receptor sequencing datasets as references. HG TMEs revealed abundant exhausted/pro-tumour immune cells with no consistent increase in expression of PD-1, PD-L1 and CTLA4 checkpoints and angiogenic genes. Additional HG TME immunophenotype characteristics included: pro-tumour tissue-resident monocytes with consistently increased expression of HAVCR2 and LAG3 checkpoints; an exhausted CD8+ T cells sub-population with stem-like progenitor gene expression; and pro-tumour tumour-associated macrophages and monocytes within the recurrent TME with the expression of TREM2. Whilst limited by a modest sample size, this study represents the largest ST-seq dataset on human ccRCC. Our study reveals that high-risk ccRCC TMEs are infiltrated by exhausted/pro-tumour immunophenotypes lacking specific checkpoint gene expression confirming that HG ccRCC TME are immunogenic but not ICI favourable.
© 2023. Nature Publishing Group UK.
Conflict of interest statement
A.M.R. was supported by an Australian Government Research Training Program Scholarship. M.S.Y.N. was supported by the Royal Brisbane and Women’s Hospital Foundation 2020 Robert and Janelle Bird Postdoctoral Research Fellowship. M.R. was supported by a Metro North Hospital and Health Service Clinical Research Fellowship. A.J.M. was supported by a Queensland Health Advancing Clinical Research Fellowship. The remaining authors declare no competing interests.
Figures

References
-
- Wei SC, Duffy CR, Allison JP. Fundamental mechanisms of immune checkpoint blockade therapy. Cancer Discov. 2018;8:1069–1086. doi: 10.1158/2159-8290.CD-18-0367. - DOI - PubMed
-
- Bedke J, et al. Updated European association of urology guidelines on renal cell carcinoma: Nivolumab plus cabozantinib joins immune checkpoint inhibition combination therapies for treatment-naïve metastatic clear-cell renal cell carcinoma. Eur. Urol. 2021;79:339–342. doi: 10.1016/j.eururo.2020.12.005. - DOI - PubMed
-
- EAU Guidelines. Edn. presented at the EAU Annual Congress Amsterdam 2022. EAU http://uroweb.org/guidelines/compilations-of-all-guidelines/ (2022).
LinkOut - more resources
Full Text Sources
Research Materials
