

Multimodal Prediction of 3- and 12-Month Outcomes in ICU Patients with Acute Disorders of Consciousness
- PMID: 37697124
- PMCID: PMC10959792
- DOI: 10.1007/s12028-023-01816-z
Multimodal Prediction of 3- and 12-Month Outcomes in ICU Patients with Acute Disorders of Consciousness
Abstract
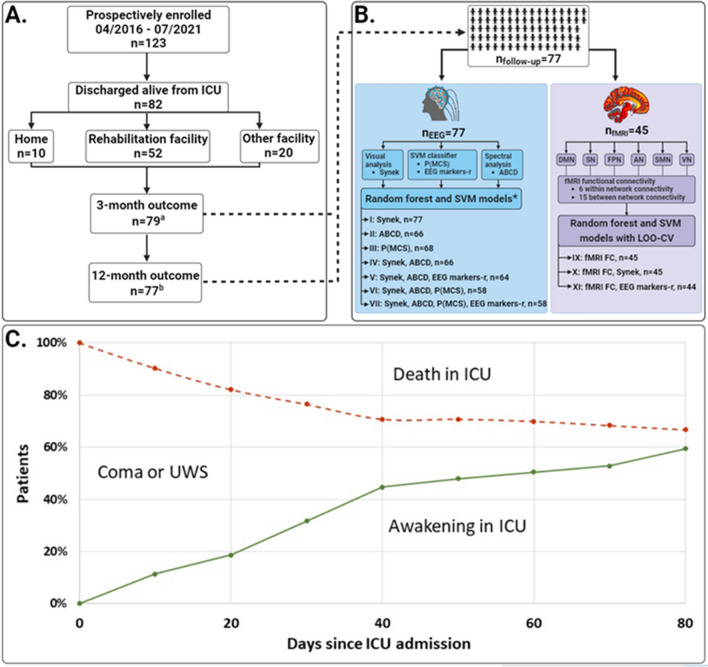
Background: In intensive care unit (ICU) patients with coma and other disorders of consciousness (DoC), outcome prediction is key to decision-making regarding prognostication, neurorehabilitation, and management of family expectations. Current prediction algorithms are largely based on chronic DoC, whereas multimodal data from acute DoC are scarce. Therefore, the Consciousness in Neurocritical Care Cohort Study Using Electroencephalography and Functional Magnetic Resonance Imaging (i.e. CONNECT-ME; ClinicalTrials.gov identifier: NCT02644265) investigates ICU patients with acute DoC due to traumatic and nontraumatic brain injuries, using electroencephalography (EEG) (resting-state and passive paradigms), functional magnetic resonance imaging (fMRI) (resting-state) and systematic clinical examinations.
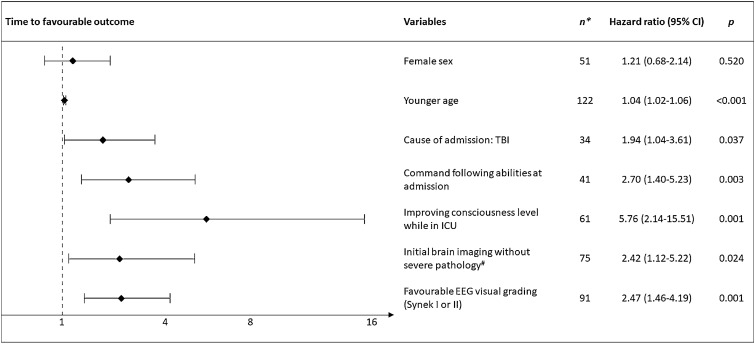
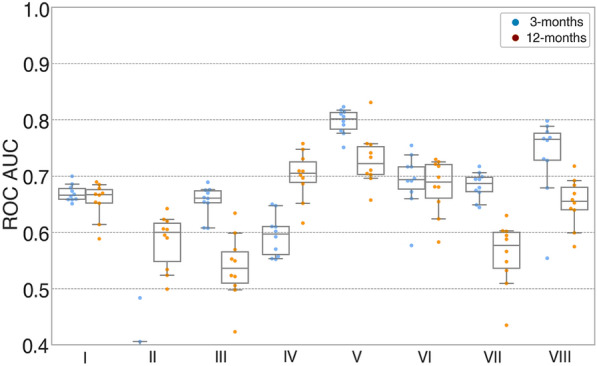
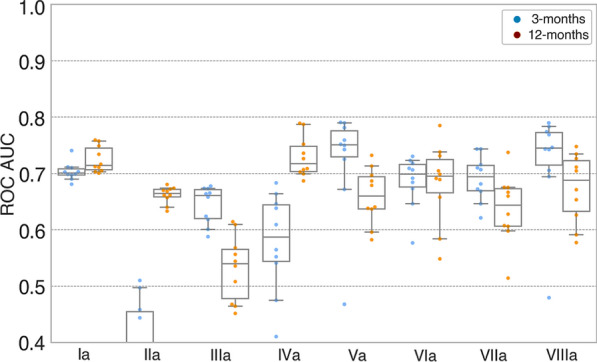
Methods: We previously presented results for a subset of patients (n = 87) concerning prediction of consciousness levels in the ICU. Now we report 3- and 12-month outcomes in an extended cohort (n = 123). Favorable outcome was defined as a modified Rankin Scale score ≤ 3, a cerebral performance category score ≤ 2, and a Glasgow Outcome Scale Extended score ≥ 4. EEG features included visual grading, automated spectral categorization, and support vector machine consciousness classifier. fMRI features included functional connectivity measures from six resting-state networks. Random forest and support vector machine were applied to EEG and fMRI features to predict outcomes. Here, random forest results are presented as areas under the curve (AUC) of receiver operating characteristic curves or accuracy. Cox proportional regression with in-hospital death as a competing risk was used to assess independent clinical predictors of time to favorable outcome.
Results: Between April 2016 and July 2021, we enrolled 123 patients (mean age 51 years, 42% women). Of 82 (66%) ICU survivors, 3- and 12-month outcomes were available for 79 (96%) and 77 (94%), respectively. EEG features predicted both 3-month (AUC 0.79 [95% confidence interval (CI) 0.77-0.82]) and 12-month (AUC 0.74 [95% CI 0.71-0.77]) outcomes. fMRI features appeared to predict 3-month outcome (accuracy 0.69-0.78) both alone and when combined with some EEG features (accuracies 0.73-0.84) but not 12-month outcome (larger sample sizes needed). Independent clinical predictors of time to favorable outcome were younger age (hazard ratio [HR] 1.04 [95% CI 1.02-1.06]), traumatic brain injury (HR 1.94 [95% CI 1.04-3.61]), command-following abilities at admission (HR 2.70 [95% CI 1.40-5.23]), initial brain imaging without severe pathological findings (HR 2.42 [95% CI 1.12-5.22]), improving consciousness in the ICU (HR 5.76 [95% CI 2.41-15.51]), and favorable visual-graded EEG (HR 2.47 [95% CI 1.46-4.19]).
Conclusions: Our results indicate that EEG and fMRI features and readily available clinical data predict short-term outcome of patients with acute DoC and that EEG also predicts 12-month outcome after ICU discharge.
Keywords: Coma; Consciousness; Electroencephalography; Functional magnetic resonance imaging; Intensive care unit.
© 2023. The Author(s).
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Owen AM, Coleman MR, Boly M, Davis MH, Laureys S, Pickard JD. Detecting awareness in the vegetative state. Science. 2006;313(5792):1402. - PubMed
-
- Ballanti S, Campagnini S, Liuzzi P, et al. EEG-based methods for recovery prognosis of patients with disorders of consciousness: a systematic review. Clin Neurophysiol. 2022;144:98–114. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
