

Enhancing European Management of Analgesia, Sedation, and Delirium: A Multinational, Prospective, Interventional Before-After Trial
- PMID: 37697129
- PMCID: PMC11147880
- DOI: 10.1007/s12028-023-01837-8
Enhancing European Management of Analgesia, Sedation, and Delirium: A Multinational, Prospective, Interventional Before-After Trial
Abstract
Background: The objective of this study was to analyze the impact of a structured educational intervention on the implementation of guideline-recommended pain, agitation, and delirium (PAD) assessment.
Methods: This was a prospective, multinational, interventional before-after trial conducted at 12 intensive care units from 10 centers in Germany, Austria, Switzerland, and the UK. Intensive care units underwent a 6-week structured educational program, comprising online lectures, instructional videos, educational handouts, and bedside teaching. Patient-level PAD assessment data were collected in three 1-day point-prevalence assessments before (T1), 6 weeks after (T2), and 1 year after (T3) the educational program.
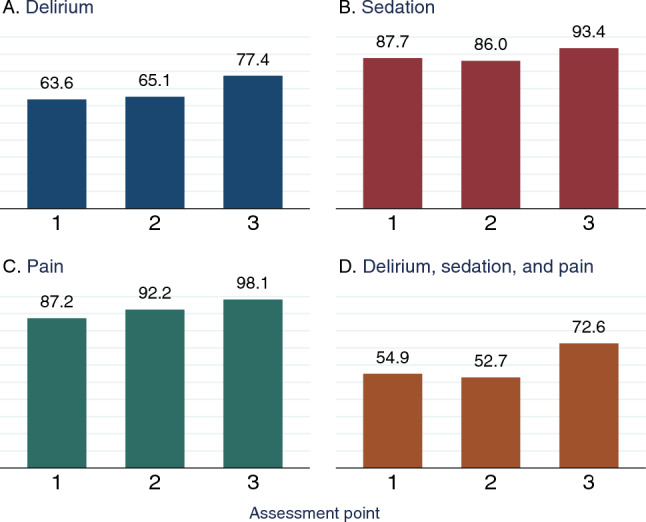
Results: A total of 430 patients were included. The rate of patients who received all three PAD assessments changed from 55% (107/195) at T1 to 53% (68/129) at T2, but increased to 73% (77/106) at T3 (p = 0.003). The delirium screening rate increased from 64% (124/195) at T1 to 65% (84/129) at T2 and 77% (82/106) at T3 (p = 0.041). The pain assessment rate increased from 87% (170/195) at T1 to 92% (119/129) at T2 and 98% (104/106) at T3 (p = 0.005). The rate of sedation assessment showed no signficiant change. The proportion of patients who received nonpharmacological delirium prevention measures increased from 58% (114/195) at T1 to 80% (103/129) at T2 and 91% (96/106) at T3 (p < 0.001). Multivariable regression revealed that at T3, patients were more likely to receive a delirium assessment (odds ratio [OR] 2.138, 95% confidence interval [CI] 1.206-3.790; p = 0.009), sedation assessment (OR 4.131, 95% CI 1.372-12.438; p = 0.012), or all three PAD assessments (OR 2.295, 95% CI 1.349-3.903; p = 0.002) compared with T1.
Conclusions: In routine care, many patients were not assessed for PAD. Assessment rates increased significantly 1 year after the intervention. Clinical trial registration ClinicalTrials.gov: NCT03553719.
Keywords: Critical care; Delirium; Delivery of health care; Europe; Intensive care units.
© 2023. The Author(s).
Conflict of interest statement
NP, JJG, MR, JH, BP, AR, UP, CS, PS, EL, and DC report no conflicts of interest. Outside the submitted work, CDS reports grants from Deutsche Forschungsgemeinschaft/German Research Society, grants from Deutsches Zentrum für Luft- und Raumfahrt e. V. (DLR)/German Aerospace Center, grants from Einstein Stiftung Berlin/Einstein Foundation Berlin, grants from Gemeinsamer Bundesausschuss/Federal Joint Committee (G-BA), grants from Inneruniversitäre Forschungsförderung/Inner University Grants, grants from Projektträger im DLR/Project Management Agency, grants from Stifterverband/Nonprofit Society Promoting Science and Education, grants from European Society of Anaesthesiology and Intensive Care, grants from BMWI (Federal Ministry for Economic Affairs and Climate Action), grants from Baxter Deutschland GmbH, grants from Cytosorbents Europe GmbH, grants from Edwards Lifesciences Germany GmbH, grants from Fresenius Medical Care, grants from Grünenthal GmbH, grants from Masimo Europe Ltd., grants from Pfizer Pharma PFE GmbH, personal fees from Georg Thieme Verlag, grants from Dr. F. Köhler Chemie GmbH, grants from Sintetica GmbH, grants from Stifterverband für die deutsche Wissenschaft e.V./Philips, grants from Stiftung Charité, grants from AGUETTANT Deutschland GmbH, grants from AbbVie Deutschland GmbH & Co. KG, grants from Amomed Pharma GmbH, grants from InTouch Health, grants from Copra System GmbH, grants from Correvio GmbH, grants from Drägerwerk AG & Co. KGaA, grants from Gemeinsamer Bundesausschuss/Federal Joint Committee (G-BA) – Innovationsfonds, grants from Max-Planck-Gesellschaft zur Förderung der Wissenschaften e.V., grants from Deutsche Gesellschaft für Anästhesiologie & Intensivmedizin (DGAI), grants from Stifterverband für die deutsche Wissenschaft e.V./Metronic, grants from Philips ElectronicsNederland BV, grants from BMBF – Federal Ministry of Education and Research, grants from BMBF/RKI, grants from Deutsche Forschungsgemeinschaft/German Research Society; in addition, CDS has a patent 15753 627.7 issued (Europe), a patent PCT/EP 2015/067731 issued (US), a patent 3 174 588 issued (Europe), a patent 10 2014 215 211.9 licensed, a patent 10 2018 114 364.8 licensed, a patent 10 2018 110 275.5 licensed, a patent 50 2015 010 534.8 licensed, a patent 50 2015 010 347.7 licensed, and a patent 10 2014 215 212.7 licensed; in addition, CDS reports a leadership role at AWMF (Association of the Scientific Medical Societies in Germany), a leadership role at Deutsche Forschungsgemeinschaft (German Research Foundation) review boards, and a leadership role at Deutsche Akademie der Naturforscher Leopoldina e.V. (German National Academy of Sciences – Leopoldina). Outside the submitted work, VJP reports a project grant from Alzheimers Society UK. Outside the submitted work, RvH reports speaker fees from OrionPharma. Outside the submitted work, CW reports fees for patient recruitment as investigator of the Sedaconda study SED001, honoraria for a presentation on a symposium for Sedana medical AB, honoraria as board member of Digimed GmbH (quality insurance software), a leadership role as editor of the journal “Notfall + Rettungsmedizin,” and a leadership role as a member of the board of directors of the DIVI (German Association of Intensive Care Medicine). Outside the submitted work, MS reports grants from Edwards Lifescience, grants from Medtronic, personal fees from Georg Thieme Verlag, honoraria from Edwards Lifescience, honoraria from BTG, honoraria from OrionPharma, a leadership role as president of MJC Intensivmedizin UEMS, a leadership role as German representative of the European Board of Anesthesiology/Section Anesthesiology of the UEMS, a member role of the ICU Subcom of ESAIC, a leadership role as corresponding author of S3-Leitlinie für die Intensivmedizin bei herzchirurgischen Patienten: Hämodynamisches Monitoring und kardiopulmonales System, and a leadership role as Schriftführer Arbeitskreis Kardioanästhesie der DGAI. Outside the submitted work, SKP reports participation on a data safety monitoring board for study German Clinical Trial Register DRKS 00021256, prospectively registered on 24.04.2020. Outside the submitted work, AT received consultation honoraria from Argenx and is a member of the medical advisory board of the German Myasthenia Society. BW reports a NEXT Start-up Grant from the European Society of Intensive Care Medicine (ESICM) related to the study; outside the submitted work, BW reports grants from Gemeinsamer Bundesausschuss / Federal Joint Committee (G-BA)—Innovationsfonds, consulting fees from OrionPharma, honoraria from Dr. F. Köhler Chemie, support for attending meetings and travel from Teladoc Health, a leadership role as ESICM NEXT Chair, a member role in the ESICM ARDS Guideline group, and a member role in the Covriin-Group of the Robert Koch Institute.
Figures

References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
