

A Solution to the Cerebral Perfusion Pressure Transducer Placement Conundrum in Neurointensive Care? The Dual Transducer
- PMID: 37697130
- PMCID: PMC10959835
- DOI: 10.1007/s12028-023-01829-8
A Solution to the Cerebral Perfusion Pressure Transducer Placement Conundrum in Neurointensive Care? The Dual Transducer
Abstract
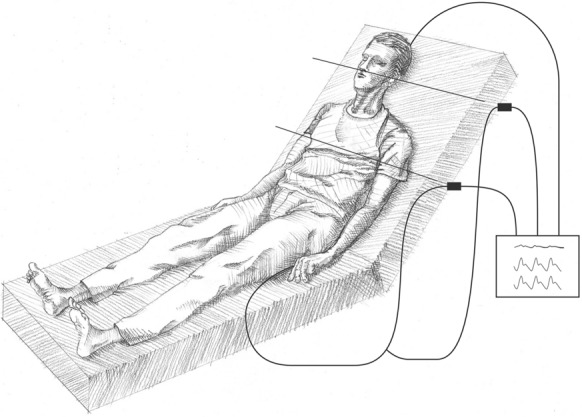
Intracranial pressure is routinely monitored in most intensive care units caring for patients with severe neurological insults and, together with continuous arterial blood pressure measurement, allows for monitoring of cerebral perfusion pressure (CPP). CPP is the driving pressure of blood flow to the brain and is used to guide therapy. However, there is considerable inconsistency in the literature regarding how CPP is technically measured and, more specifically, the appropriate placement of the arterial pressure transducer. Depending on patient positioning and where the arterial pressure transducer is placed, the mean arterial pressure used for CPP calculation can vary widely by up to 15 mm Hg, which is greater than the acceptable variation in target ranges used clinically. Physiologically, the arterial pressure transducer should be placed at the level of the foramen of Monro for CPP measurement, but it is commonly set at the level of the right atrium for systematic measurement. Mean arterial pressure measurement at the level of the right atrium can lead to overestimation and potentially critically low actual CPP levels when the head is elevated, and measurement at the level of the foramen of Monro will underestimate systemic pressures, increasing the risk of excessive and unnecessary use of vasopressors and fluid. At the Karolinska University Hospital neurointensive care unit, we have used a split dual-transducer system, measuring arterial pressure both at the level of the foramen of Monro and at the level of the right atrium from a single arterial source. In doing so, we work with constants and can monitor and target optimum arterial pressures to better secure perfusion to all organs, with potentially less risk of cerebral ischemia or overuse of vasopressors and fluids, which may affect outcome.
Keywords: 1. Background; Brain injury; Cerebrovascular monitoring; Critical care; Intracranial pressure; Patient monitoring; Pressure; Transducers.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Sahuquillo J, Munar F, Baguena M, Poca MA, Pedraza S, Rodríguez-Baeza A. Evaluation of cerebrovascular CO2-reactivity and autoregulation in patients with post-traumatic diffuse brain swelling (diffuse injury III) Acta Neurochir Suppl. 1998;71:233–236. - PubMed
-
- Carney N, Totten AM, O'Reilly C, et al. Guidelines for the management of severe traumatic brain injury. 4th ed. Palo Alto (CA): Brain Trauma Foundation; 2016.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
