

The course of health-related quality of life after the diagnosis of childhood cancer: a national cohort study
- PMID: 37697253
- PMCID: PMC10496372
- DOI: 10.1186/s12885-023-11379-z
The course of health-related quality of life after the diagnosis of childhood cancer: a national cohort study
Abstract
Background: Comprehensive insight in the longitudinal development of health-related quality of life (HRQOL) after childhood cancer diagnosis could improve quality of care. Thus, we aimed to study the course and biopsychosocial determinants of HRQOL in a unique national cohort of children with cancer.
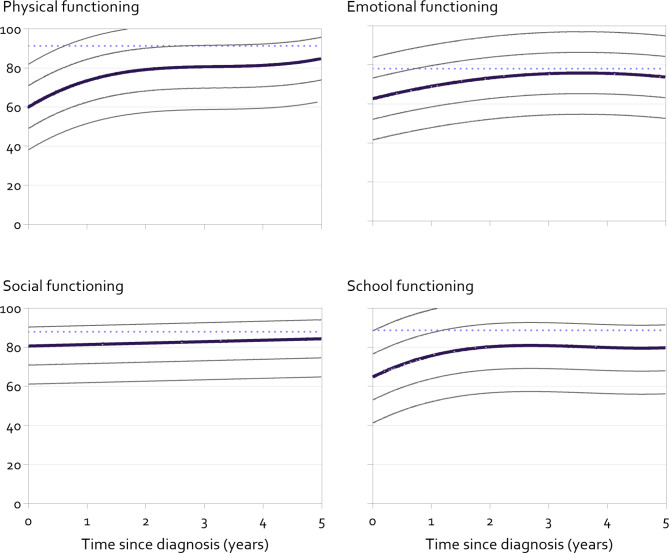
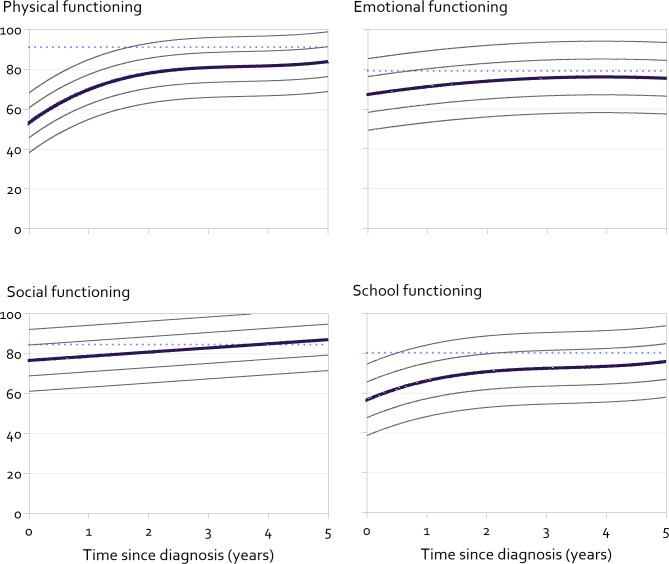
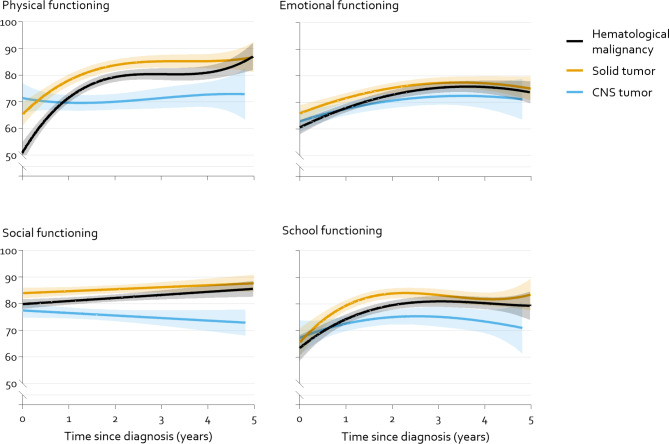
Methods: HRQOL of 2154 children with cancer was longitudinally reported (median: 3 reports) between diagnosis and 5 years after, using the pediatric quality of life inventory generic core scales (PedsQL). HRQOL was modelled over time since diagnosis using mixed model analysis for children 2-7 years (caregiver-reports) and ≥ 8 years (self-reports). Differences in the course between hematological, solid and central nervous system malignancies were studied. Additional associations of demographics, disease characteristics (age at diagnosis, relapse, diagnosis after the national centralization of childhood cancer care and treatment components) and caregiver distress (Distress thermometer) were studied.
Results: Overall, HRQOL improved with time since diagnosis, mostly in the first years. The course of HRQOL differed between diagnostic groups. In children aged 2-7 years, children with a solid tumor had most favorable HRQOL. In children aged ≥ 8 years, those with a hematological malignancy had lower HRQOL around diagnosis, but stronger improvement over time than the other diagnostic groups. In both age-groups, the course of HRQOL of children with a CNS tumor showed little or no improvement. Small to moderate associations (β: 0.18 to 0.67, p < 0.05) with disease characteristics were found. Centralized care related to better HRQOL (β: 0.25 to 0.44, p < 0.05). Caregiver distress was most consistently associated with worse HRQOL (β: - 0.13 to - 0.48, p < 0.01).
Conclusions: The HRQOL course presented can aid in identifying children who have not fully recovered their HRQOL following cancer diagnosis, enabling early recognition of the issue. Future research should focus on ways to support children, especially those with a CNS tumor, for example by decreasing distress in their caregivers.
Keywords: Central nervous system tumor; Childhood cancer; Emotional functioning; Health-related quality of life; Longitudinal study; Parental distress; Physical functioning; Social functioning.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Kazak AE, Abrams AN, Banks J, Christofferson J, DiDonato S, Grootenhuis MA, et al. Psychosocial Assessment as a Standard of Care in Pediatric Cancer. Pediatr Blood Cancer. 2015;62(Suppl 5):426–59. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
