

Empiric antimicrobial therapy in the intensive care unit based on the risk of multidrug-resistant bacterial infection: a single-centre case‒control study of blood culture results in Japan
- PMID: 37697404
- PMCID: PMC10496235
- DOI: 10.1186/s13756-023-01303-2
Empiric antimicrobial therapy in the intensive care unit based on the risk of multidrug-resistant bacterial infection: a single-centre case‒control study of blood culture results in Japan
Abstract
Background: Infections and sepsis are the leading causes of death in intensive care units (ICUs). Antimicrobial agent selection is challenging because the intervention is directly related to the outcome, and the problem of antimicrobial resistance (AMR) must be considered. Therefore, in this study, we aimed to clarify the epidemiological data and examine whether the detection rate of multidrug-resistant (MDR) bacteria differed depending on the presence or absence of the risk of MDR bacterial infections to establish guidance regarding the choice of antimicrobial therapy for ICU patients.
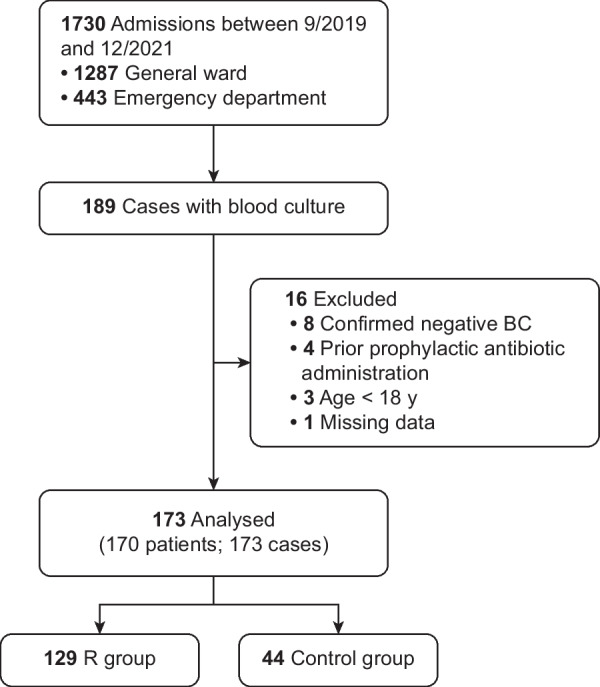
Methods: This retrospective case‒control study was performed in a single ICU in Japan. Patients admitted to the ICU who underwent blood culture (BC) analysis were considered for inclusion in this study; patients were at risk of MDR bacterial infections, and controls were not. The primary outcome measure was the detection rate of MDR bacteria in BCs collected from patients and controls. The secondary outcome measure was the selection rate of anti-Pseudomonas and anti-methicillin-resistant Staphylococcus aureus (MRSA) drugs for patients and controls.
Results: Among the 1,730 patients admitted to the ICU during the study period, BCs were obtained from 186 patients, and 173 samples were finally included in the analysis (n = 129 cases; n = 44 controls). No MDR bacteria or Pseudomonas aeruginosa were detected in the controls (14 (11%) vs. 0 (0%)) (P = 0.014) However, there was no difference in empiric antimicrobials, including anti-MRSA (30 (23%) vs. 12 (27%)) (P = 0.592) and anti-Pseudomonas aeruginosa (61 (47%) vs. 16 (36%)) (P = 0.208) drugs, that were administered to the two groups.
Conclusions: Even in critically ill patients in the ICU, MDR bacteria are unlikely to be detected in patients without the risk of MDR bacterial infections. Therefore, for such patients, a strategy of starting empiric narrow-spectrum antimicrobial therapy rather than empiric broad-spectrum therapy should be considered. This strategy, in conjunction with daily updates of clinical and epidemiological data at each facility, will promote the appropriate use of antimicrobials and reduce the emergence of MDR bacteria in the ICU.
Trial registration: None.
Keywords: Bacteraemia; Blood culture; Empiric therapy; Multidrug-resistant bacteria; Pseudomonas aeruginosa; Sepsis.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Tabah A, Koulenti D, Laupland K, Misset B, Valles J, De Carvalho FB, et al. Characteristics and determinants of outcome of hospital-acquired bloodstream infections in intensive care units: the EUROBACT international cohort study. Intensive Care Med. 2012;38:1930–1945. doi: 10.1007/s00134-012-2695-9. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
