

Hospital Readmissions Among Persons With Human Immunodeficiency Virus in the United States and Canada, 2005-2018: A Collaboration of Cohort Studies
- PMID: 37697938
- PMCID: PMC10733730
- DOI: 10.1093/infdis/jiad396
Hospital Readmissions Among Persons With Human Immunodeficiency Virus in the United States and Canada, 2005-2018: A Collaboration of Cohort Studies
Abstract
Background: Hospital readmission trends for persons with human immunodeficiency virus (PWH) in North America in the context of policy changes, improved antiretroviral therapy (ART), and aging are not well-known. We examined readmissions during 2005-2018 among adult PWH in NA-ACCORD.
Methods: Linear risk regression estimated calendar trends in 30-day readmissions, adjusted for demographics, CD4 count, AIDS history, virologic suppression (<400 copies/mL), and cohort.
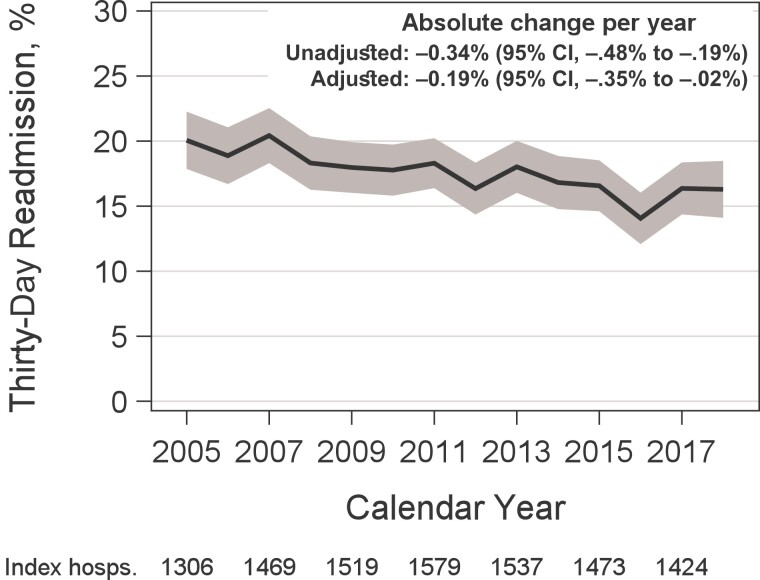
Results: We examined 20 189 hospitalizations among 8823 PWH (73% cisgender men, 38% White, 38% Black). PWH hospitalized in 2018 versus 2005 had higher median age (54 vs 44 years), CD4 count (469 vs 274 cells/μL), and virologic suppression (83% vs 49%). Unadjusted 30-day readmissions decreased from 20.1% (95% confidence interval [CI], 17.9%-22.3%) in 2005 to 16.3% (95% CI, 14.1%-18.5%) in 2018. Absolute annual trends were -0.34% (95% CI, -.48% to -.19%) in unadjusted and -0.19% (95% CI, -.35% to -.02%) in adjusted analyses. By index hospitalization reason, there were significant adjusted decreases only for cardiovascular and psychiatric hospitalizations. Readmission reason was most frequently in the same diagnostic category as the index hospitalization.
Conclusions: Readmissions decreased over 2005-2018 but remained higher than the general population's. Significant decreases after adjusting for CD4 count and virologic suppression suggest that factors alongside improved ART contributed to lower readmissions. Efforts are needed to further prevent readmissions in PWH.
Keywords: HIV; aging; healthcare utilization; hospitalization; readmission.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. K. N. A. reports grants to their institution from NIH; royalties or licenses from Coursera; and consulting fees from NIH and TrioHealth. R. J. B. reports grants to their institution from NIH and support for travel from NIH. J. A. C. reports grants to their institution from NIH and payment or honoraria from Prime Education and Integritas Communications. H. M. C. reports grants to their institution from AHRQ, NIH, and ViiV Healthcare; and participation in a data and safety monitoring board (DSMB) or advisory board for Gilead Sciences, NIH Office of AIDS Research, and ViiV Healthcare. J. J. E. reports grants to their institution from NIH, ViiV Healthcare, Gilead Sciences, and Janssen; consulting fees from ViiV Healthcare, Gilead Sciences, and Merck & Co; and participation on a DSMB or advisory board for TAIMED. K. A. G. reports grants to their institution from the US Department of Defense, NIH, Mental Wellness Foundation, HealthNetwork Foundation, Bloomberg Philanthropies, Defense Health Agency, the State of Maryland, Octapharma, Moriah Fund, and National Center for Advancing Translational Sciences; consulting fees from Spark HealthCare, Teach for America, and Aspen Institute; and participation on a DSMB or advisory board for Pfizer. M. J. G. reports grants to their institution from NIH; and participation on a DSMB or advisor board for Merck & Co, Gilead Sciences, and ViiV Healthcare. B. C. H. reports grants to their institution from NIH. M. A. H. reports grants to their institution from NIH. M. Y. K. reports grants to their institution from Gilead Sciences and ViiV Healthcare; payment or honoraria to their institution from Practice Point Communications CME; leadership in the AIDS Clinical Trials Group (ACTG) Underrepresented Populations Committee (Vice Chair) with payments to their institution; and uncompensated leadership on the Being Alive San Diego Board (member). M. B. K. reports grants to their institution from NIH, ViiV Healthcare, AbbVie, and Gilead Sciences; and consulting fees from ViiV Healthcare, AbbVie, and Gilead Sciences. R. L. reports support for travel from CIHR. V. D. L. reports grants to their institution from CIHR; payment or honoraria from ViiV Healthcare; support for travel from the Conference on Retroviruses and Opportunistic Infections; and participation on a DSMB or advisory board for the Providence Health Care Ethics Board. R. D. M. reports grants to their institution from NIH. S. N. reports grants to their institution from NIH. A. N. reports grants to their institution from Gilead Sciences. P. F. R. reports grants to their institution from NIH and consulting fees from Gilead Sciences and Janssen. J. E. T. reports grants to their institution from the National Eye Institute and ACTG; consulting fees from Gilead Sciences, Canfield, and UpToDate; participation on a DSMB or advisory board for NEI and Tarsier; stock or stock options in Tarsier; and fees for serving as Editor-in-Chief for Ocular Immunology and Inflammation. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Feller DJ, Akiyama MJ, Gordon P, Agins BD. Readmissions in HIV-infected inpatients: a large cohort analysis. J Acquir Immune Defic Syndr 2016; 71:407–12. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DA036935/DA/NIDA NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
- NH/NIH HHS/United States
- K01 HL169020/HL/NHLBI NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- CC/CDC HHS/United States
- K01 AI093197/AI/NIAID NIH HHS/United States
- F31 AI124794/AI/NIAID NIH HHS/United States
- F31 DA037788/DA/NIDA NIH HHS/United States
- G12 MD007583/MD/NIMHD NIH HHS/United States
- K01 AI093197/AI/NIAID NIH HHS/United States
- K01 AI131895/AI/NIAID NIH HHS/United States
- K23 EY013707/EY/NEI NIH HHS/United States
- K24 AI065298/AI/NIAID NIH HHS/United States
- K24 AI118591/AI/NIAID NIH HHS/United States
- K24 DA000432/DA/NIDA NIH HHS/United States
- KL2 TR000421/TR/NCATS NIH HHS/United States
- N01 CP001004/CP/NCI NIH HHS/United States
- N02 CP055504/CP/NCI NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- P30 AI027767/AI/NIAID NIH HHS/United States
- P30 AI036219/AI/NIAID NIH HHS/United States
- P30 AI050409/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- P30 AI094189/AI/NIAID NIH HHS/United States
- P30 AI110527/AI/NIAID NIH HHS/United States
- P30 MH062246/MH/NIMH NIH HHS/United States
- R01 AA016893/AA/NIAAA NIH HHS/United States
- R01 DA011602/DA/NIDA NIH HHS/United States
- R01 DA012568/DA/NIDA NIH HHS/United States
- R01 AG053100/AG/NIA NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- R34 DA045592/DA/NIDA NIH HHS/United States
- U01 AA013566/AA/NIAAA NIH HHS/United States
- U01 AA020790/AA/NIAAA NIH HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- U01 AI069434/AI/NIAID NIH HHS/United States
- U01 DA036297/DA/NIDA NIH HHS/United States
- U10 EY008057/EY/NEI NIH HHS/United States
- U10 EY008052/EY/NEI NIH HHS/United States
- U10 EY008067/EY/NEI NIH HHS/United States
- U01 HL146192/HL/NHLBI NIH HHS/United States
- U01 HL146193/HL/NHLBI NIH HHS/United States
- U01 HL146194/HL/NHLBI NIH HHS/United States
- U01 HL146201/HL/NHLBI NIH HHS/United States
- U01 HL146202/HL/NHLBI NIH HHS/United States
- U01 HL146203/HL/NHLBI NIH HHS/United States
- U01 HL146204/HL/NHLBI NIH HHS/United States
- U01 HL146205/HL/NHLBI NIH HHS/United States
- U01 HL146208/HL/NHLBI NIH HHS/United States
- U01 HL146240/HL/NHLBI NIH HHS/United States
- U01 HL146241/HL/NHLBI NIH HHS/United States
- U01 HL146242/HL/NHLBI NIH HHS/United States
- U01 HL146245/HL/NHLBI NIH HHS/United States
- U01 HL146333/HL/NHLBI NIH HHS/United States
- U24 AA020794/AA/NIAAA NIH HHS/United States
- U54 GM133807/GM/NIGMS NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- UL1 TR000083/TR/NCATS NIH HHS/United States
- UL1 TR002378/TR/NCATS NIH HHS/United States
- Z01 CP010176/ImNIH/Intramural NIH HHS/United States
- T32 DA007250/DA/NIDA NIH HHS/United States
- CIHR/Canada
