

Outcomes of patients aged ≥80 years with respiratory failure initially treated with non-invasive ventilation in European intensive care units before and during COVID-19 pandemic
- PMID: 37698708
- PMCID: PMC10497468
- DOI: 10.1186/s13613-023-01173-2
Outcomes of patients aged ≥80 years with respiratory failure initially treated with non-invasive ventilation in European intensive care units before and during COVID-19 pandemic
Abstract
Background: Non-invasive ventilation (NIV) has been commonly used to treat acute respiratory failure due to COVID-19. In this study we aimed to compare outcomes of older critically ill patients treated with NIV before and during the COVID-19 pandemic.
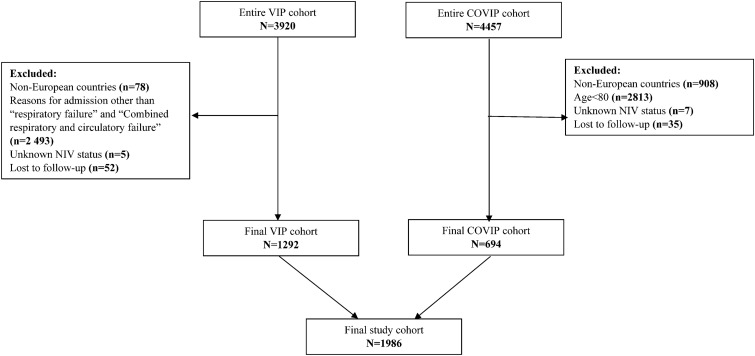
Methods: We analysed a merged cohort of older adults admitted to intensive care units (ICUs) due to respiratory failure. Patients were enrolled into one of two prospective observational studies: before COVID-19 (VIP2-2018 to 2019) and admitted due to COVID-19 (COVIP-March 2020 to January 2023). The outcomes included: 30-day mortality, intubation rate and NIV failure (death or intubation within 30 days).
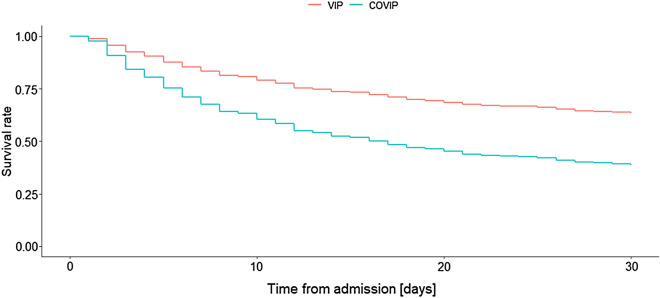
Results: The final cohort included 1986 patients (1292 from VIP2, 694 from COVIP) with a median age of 83 years. NIV was used as a primary mode of respiratory support in 697 participants (35.1%). ICU admission due to COVID-19 was associated with an increased 30-day mortality (65.5% vs. 36.5%, HR 2.18, 95% CI 1.71 to 2.77), more frequent intubation (36.9% vs. 17.5%, OR 2.63, 95% CI 1.74 to 3.99) and NIV failure (76.2% vs. 45.3%, OR 4.21, 95% CI 2.84 to 6.34) compared to non-COVID causes of respiratory failure. Sensitivity analysis after exclusion of patients in whom life supporting treatment limitation was introduced during primary NIV confirmed higher 30-day mortality in patients with COVID-19 (52.5% vs. 23.4%, HR 2.64, 95% CI 1.83 to 3.80).
Conclusion: The outcomes of patients aged ≥80 years treated with NIV during COVID-19 pandemic were worse compared then those treated with NIV in the pre-pandemic era.
Keywords: COVID-19; Intensive care unit; Non-invasive ventilation; Older patients; Respiratory failure.
© 2023. La Société de Réanimation de Langue Francaise = The French Society of Intensive Care (SRLF).
Conflict of interest statement
Joerg C. Schefold declares that the Dept. of Intensive Care Medicine Bern has/had research and/or development/consulting contracts with (full disclosure): Orion Corporation, Abbott Nutrition International, B. Braun Medical AG, CSEM SA, Edwards Lifesciences Services GmbH/SA, Kenta Biotech Ltd, Maquet Critical Care AB, Omnicare Clinical Research AG, and Nestlé. Educational grants were received from Fresenius Kabi; GSK; MSD; Lilly; Baxter; Astellas; AstraZeneca; B. Braun Medical AG, CSL Behring, Maquet, Novartis, Covidien, Nycomed, Pierre Fabre Pharma (Roba Pharma); Pfizer, Orion Pharma. The money went into departmental funds. No personal financial gain applies. All other authors do not have any conflict of interest to declare related to this manuscript.
Figures

References
-
- Cammarota G, Esposito T, Azzolina D, Cosentini R, Menzella F, Aliberti S, et al. Noninvasive respiratory support outside the intensive care unit for acute respiratory failure related to coronavirus-19 disease: a systematic review and meta-analysis. Crit Care. 2021;25(1):268. doi: 10.1186/s13054-021-03697-0. - DOI - PMC - PubMed
