

Factors Influencing Surgical Decision-Making in the Posterior Laminectomy With Fixation for Degenerative Cervical Myelopathy (POLYFIX-DCM) Trial: Survey Study
- PMID: 37698903
- PMCID: PMC10523224
- DOI: 10.2196/48321
Factors Influencing Surgical Decision-Making in the Posterior Laminectomy With Fixation for Degenerative Cervical Myelopathy (POLYFIX-DCM) Trial: Survey Study
Abstract
Background: Degenerative cervical myelopathy (DCM) is estimated to affect 2% of the adult population. DCM occurs when degenerative processes cause compression and injure the spinal cord. Surgery to remove the stress caused by the compression of the spinal cord is the mainstay of treatment, with a range of techniques in use. Although various factors are described to inform the selection of these techniques, there needs to be more consensus and limited comparative evidence.
Objective: The main objective of this survey was to explore the variation of practice and decision-making, with a focus on laminectomy versus laminectomy and fusion in posterior surgery of the cervical spine. We present the results of a survey conducted among the principal investigators (PIs) of the National Institute for Health and Care Research (NIHR) randomized controlled trial on posterior laminectomy with fixation for degenerative cervical myelopathy (POLYFIX-DCM).
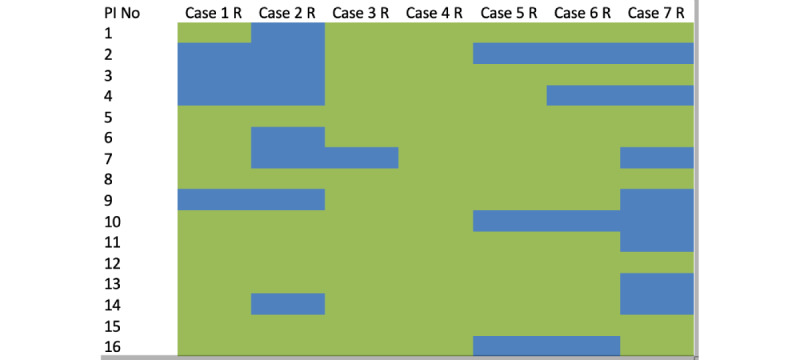
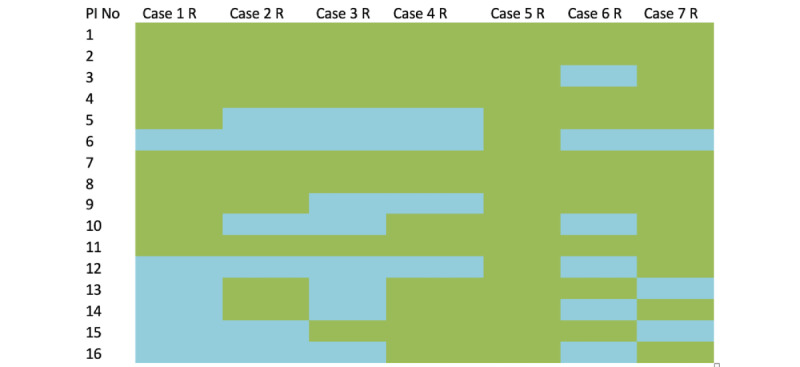
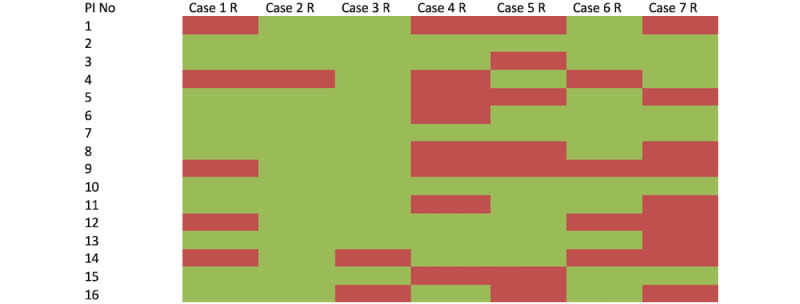
Methods: A series of 7 cases were shared with 24 PIs using SurveyMonkey. Each case consisted of a midsagittal T2-weighted magnetic resonance imaging and lateral cervical x-rays in flexion and extension. Surgeons were asked if their preferred approach was anterior or posterior. If posterior, they were asked whether they preferred to instrument and whether they had the equipoise to randomize in the NIHR POLYFIX-DCM trial. Variability in decision-making was then explored using factors reported to inform decision-making, such as alignment, location of compression, number of levels operated, presence of mobile spondylolisthesis, and patient age.
Results: The majority of PIs (16/30, 53%) completed the survey. Overall, PIs favored a posterior approach (12/16, 75%) with instrumentation (75/112, average 66%) and would randomize (67/112, average 62%) most cases. Factors reported to inform decision-making poorly explained variability in responses in both univariate testing and with a multivariate model (R2=0.1). Only surgeon experience of more than 5 years and orthopedic specialty training background were significant predictors, both associated with an anterior approach (odds ratio [OR] 1.255; P=.02 and OR 1.344; P=.007, respectively) and fusion for posterior procedures (OR 0.628; P<.001 and OR 1.344; P<.001, respectively). Surgeon experience also significantly affected the openness to randomize, with those with more than 5 years of experience less likely to randomize (OR -0.68; P<.001).
Conclusions: In this representative sample of spine surgeons participating in the POLYFIX-DCM trial as investigators, there is no consensus on surgical strategy, including the role of instrumented fusion following posterior decompression. Overall, this study supports the view that there appears to be a clinical equipoise, and conceptually, a randomized controlled trial appears feasible, which sets the scene for the NIHR POLYFIX-DCM trial.
Keywords: cervical myelopathy; decision-making; decompression; degeneration; disability; disc herniation; laminectomy; myelopathy; ossification posterior longitudinal ligament; questionnaire; recovery; spinal cord; spondylosis; spondylotic stenosis; stress; surgeons; surgery.
©Stefan Yordanov, Xiaoyu Yang, Oliver Mowforth, Andreas K Demetriades, Marcel Ivanov, Pierluigi Vergara, Adrian Gardner, Erlick Pereira, Antony Bateman, Alexander Alamri, Jibin Francis, Rikin Trivedi, Mark Kotter, Benjamin Davies, Alexandru Budu, POLYFIX-DCM research Collaborative Group. Originally published in JMIR Formative Research (https://formative.jmir.org), 12.09.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Davies B, Francis J, Butler M, Mowforth O, Goacher E, Starkey Michelle, Kolias Angelos, Wynne-Jones Guy, Hutton Mike, Selvanathan Senthil, Thomson Simon, Laing Rodney J C, Hutchinson Peter J, Kotter Mark R N. Current surgical practice for multi-level degenerative cervical myelopathy: findings from an international survey of spinal surgeons. J Clin Neurosci. 2021 May;87:84–88. doi: 10.1016/j.jocn.2021.01.049.S0967-5868(21)00066-7 - DOI - PubMed
-
- Fehlings MG, Tetreault LA, Riew KD, Middleton JW, Aarabi B, Arnold PM, Brodke DS, Burns AS, Carette S, Chen R, Chiba K, Dettori JR, Furlan JC, Harrop JS, Holly LT, Kalsi-Ryan S, Kotter M, Kwon BK, Martin AR, Milligan J, Nakashima H, Nagoshi N, Rhee J, Singh A, Skelly AC, Sodhi S, Wilson JR, Yee A, Wang JC. A clinical practice guideline for the management of patients with degenerative cervical myelopathy: recommendations for patients with mild, moderate, and severe disease and nonmyelopathic patients with evidence of cord compression. Global Spine J. 2017 Sep 05;7(3 Suppl):70S–83S. doi: 10.1177/2192568217701914. https://journals.sagepub.com/doi/abs/10.1177/2192568217701914?url_ver=Z3... 10.1177_2192568217701914 - DOI - PMC - PubMed
-
- Smith S, Stewart M, Davies B, Kotter MRN. The prevalence of asymptomatic and symptomatic spinal cord compression on magnetic resonance imaging: a systematic review and meta-analysis. Global Spine J. 2021 May;11(4):597–607. doi: 10.1177/2192568220934496. https://journals.sagepub.com/doi/abs/10.1177/2192568220934496?url_ver=Z3... - DOI - PMC - PubMed
-
- Banerjee A, Mowforth OD, Nouri A, Budu A, Newcombe V, Kotter MR, Davies BM. The prevalence of degenerative cervical myelopathy-related pathologies on magnetic resonance imaging in healthy/asymptomatic individuals: a meta-analysis of published studies and comparison to a symptomatic cohort. J Clin Neurosci. 2022 May;99:53–61. doi: 10.1016/j.jocn.2022.03.002.S0967-5868(22)00094-7 - DOI - PubMed
LinkOut - more resources
Full Text Sources
