

Ultrasensitive Detection of Circulating LINE-1 ORF1p as a Specific Multicancer Biomarker
- PMID: 37698949
- PMCID: PMC10773488
- DOI: 10.1158/2159-8290.CD-23-0313
Ultrasensitive Detection of Circulating LINE-1 ORF1p as a Specific Multicancer Biomarker
Erratum in
-
Correction: Ultrasensitive Detection of Circulating LINE-1 ORF1p as a Specific Multicancer Biomarker.Cancer Discov. 2024 Sep 4;14(9):1756. doi: 10.1158/2159-8290.CD-24-0862. Cancer Discov. 2024. PMID: 39228301 Free PMC article. No abstract available.
Abstract
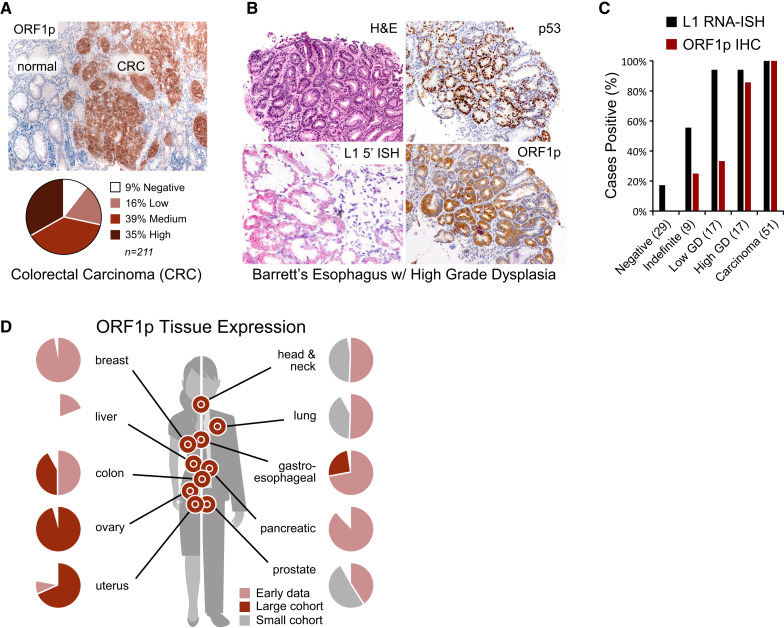
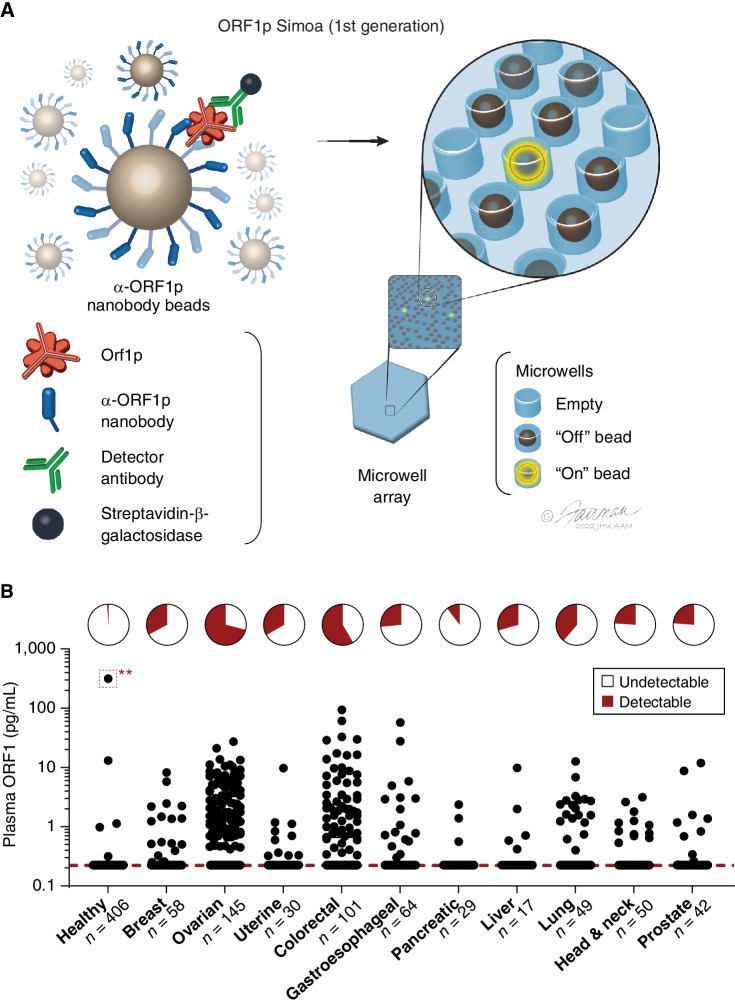
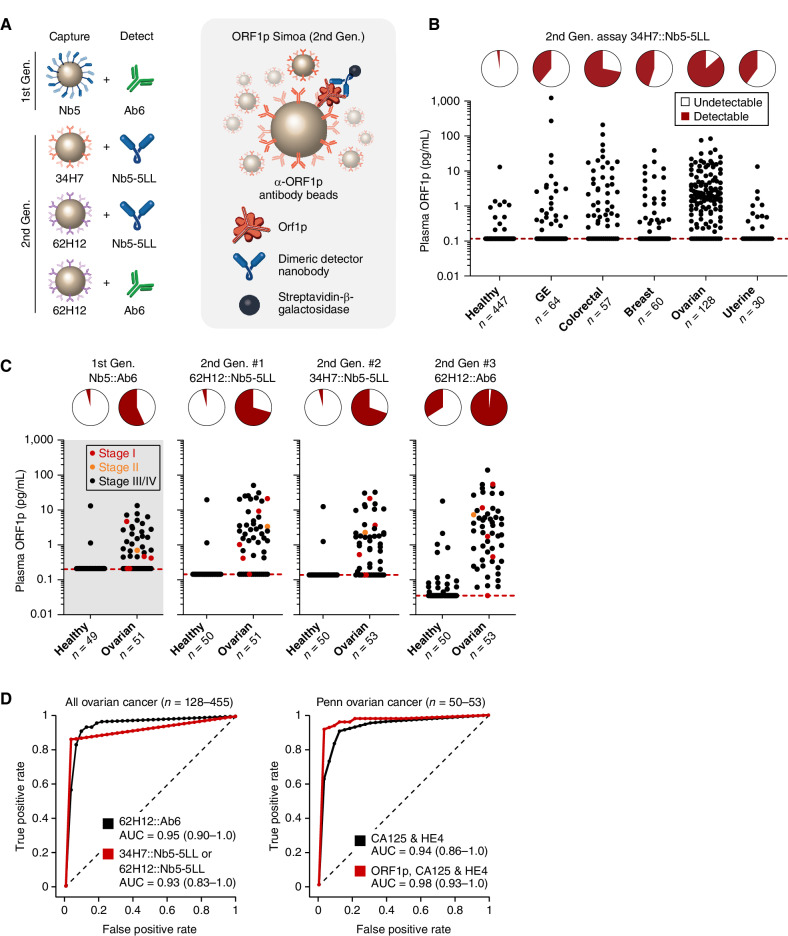
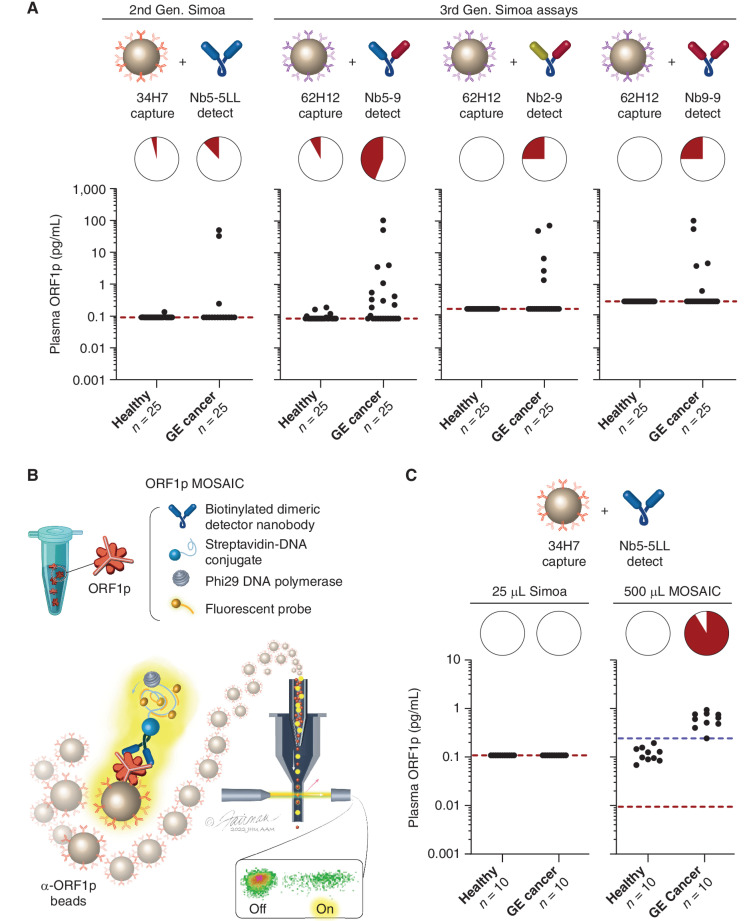
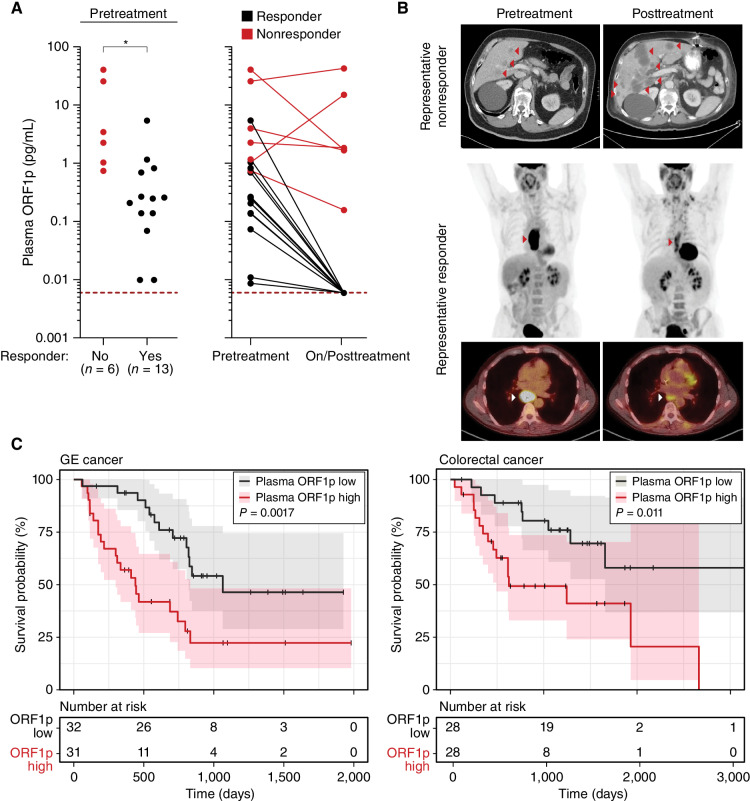
Improved biomarkers are needed for early cancer detection, risk stratification, treatment selection, and monitoring treatment response. Although proteins can be useful blood-based biomarkers, many have limited sensitivity or specificity for these applications. Long INterspersed Element-1 (LINE-1) open reading frame 1 protein (ORF1p) is a transposable element protein overexpressed in carcinomas and high-risk precursors during carcinogenesis with negligible expression in normal tissues, suggesting ORF1p could be a highly specific cancer biomarker. To explore ORF1p as a blood-based biomarker, we engineered ultrasensitive digital immunoassays that detect mid-attomolar (10-17 mol/L) ORF1p concentrations in plasma across multiple cancers with high specificity. Plasma ORF1p shows promise for early detection of ovarian cancer, improves diagnostic performance in a multianalyte panel, provides early therapeutic response monitoring in gastroesophageal cancers, and is prognostic for overall survival in gastroesophageal and colorectal cancers. Together, these observations nominate ORF1p as a multicancer biomarker with potential utility for disease detection and monitoring.
Significance: The LINE-1 ORF1p transposon protein is pervasively expressed in many cancers and is a highly specific biomarker of multiple common, lethal carcinomas and their high-risk precursors in tissue and blood. Ultrasensitive ORF1p assays from as little as 25 μL plasma are novel, rapid, cost-effective tools in cancer detection and monitoring. See related commentary by Doucet and Cristofari, p. 2502. This article is featured in Selected Articles from This Issue, p. 2489.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
![Figure 4. Targeted proteomics measurements of plasma ORF1p from large sample volumes. A, ORF1p measured from two gastric cancer patients using two quantotypic peptides (LSFISEGEIK and NLEECIR, red traces) with internal isotopically labeled standards (blue traces); a high-ORF1p cancer patient [1,231 pg/mL by Simoa, 3.5 mL plasma used for immunoprecipitation (IP)] and high-ORF1p healthy patient (3.0 pg/mL by Simoa, 5 mL plasma used for IP) are shown with 900 amol standard injected. B, Correlation between measured ORF1p by Simoa and targeted proteomics assays; r = 0.97 (Simoa vs. LSFISEGEIK) and r = 0.99 (Simoa vs. NLEECIR, t test), P < 0.0001 for both.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/3c82/10773488/dc4c7dfe3e23/2532fig4.jpg)
Update of
-
Ultrasensitive detection of circulating LINE-1 ORF1p as a specific multi-cancer biomarker.bioRxiv [Preprint]. 2023 Mar 17:2023.01.25.525462. doi: 10.1101/2023.01.25.525462. bioRxiv. 2023. Update in: Cancer Discov. 2023 Dec 12;13(12):2532-2547. doi: 10.1158/2159-8290.CD-23-0313. PMID: 36747644 Free PMC article. Updated. Preprint.
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7–33. - PubMed
-
- Sawyers CL. The cancer biomarker problem. Nature 2008;452:548–52. - PubMed
-
- Crosby D, Bhatia S, Brindle KM, Coussens LM, Dive C, Emberton M, et al. Early detection of cancer. Science 2022;375:eaay9040. - PubMed
-
- Jamshidi A, Liu MC, Klein EA, Venn O, Hubbell E, Beausang JF, et al. Evaluation of cell-free DNA approaches for multi-cancer early detection. Cancer Cell 2022;40:1537–49. - PubMed
MeSH terms
Substances
Grants and funding
- R01 CA240924/CA/NCI NIH HHS/United States
- P50 CA240243/CA/NCI NIH HHS/United States
- F32 EB029777/EB/NIBIB NIH HHS/United States
- R01 CA276112/CA/NCI NIH HHS/United States
- P50 CA228991/CA/NCI NIH HHS/United States
- T32 CA009216/CA/NCI NIH HHS/United States
- U2C CA271871/CA/NCI NIH HHS/United States
- R01 CA240816/CA/NCI NIH HHS/United States
- U01 CA228963/CA/NCI NIH HHS/United States
- P50 CA127003/CA/NCI NIH HHS/United States
- P30 CA006516/CA/NCI NIH HHS/United States
- P41 GM109824/GM/NIGMS NIH HHS/United States
- R01 GM130680/GM/NIGMS NIH HHS/United States
- K08 DK129824/DK/NIDDK NIH HHS/United States
- U01 CA152990/CA/NCI NIH HHS/United States
- R01 GM126170/GM/NIGMS NIH HHS/United States
- U01 CA233364/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
