

Eleven years of alloimmunization in 6496 patients with sickle cell disease in France who received transfusion
- PMID: 37699002
- PMCID: PMC10790094
- DOI: 10.1182/bloodadvances.2022009328
Eleven years of alloimmunization in 6496 patients with sickle cell disease in France who received transfusion
Abstract
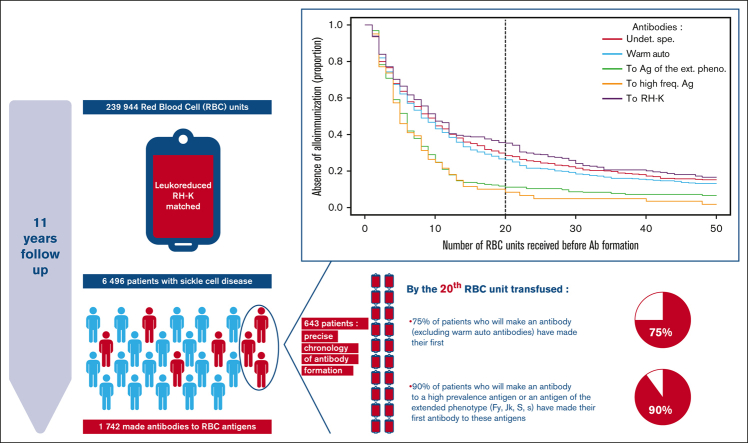
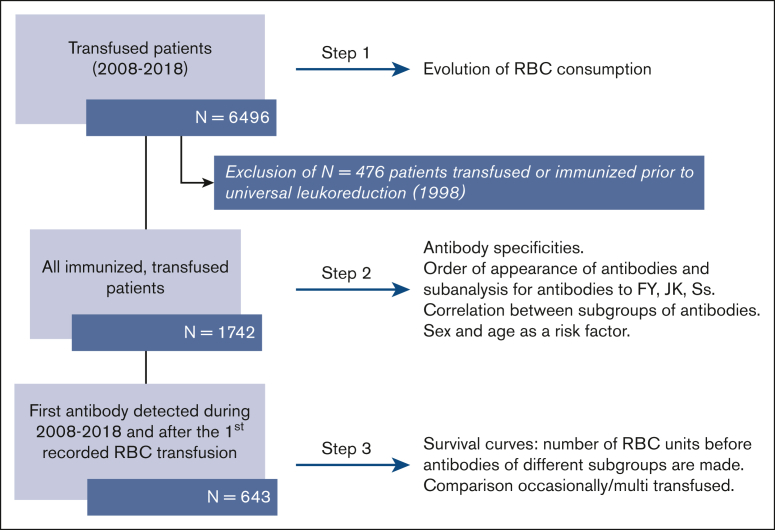
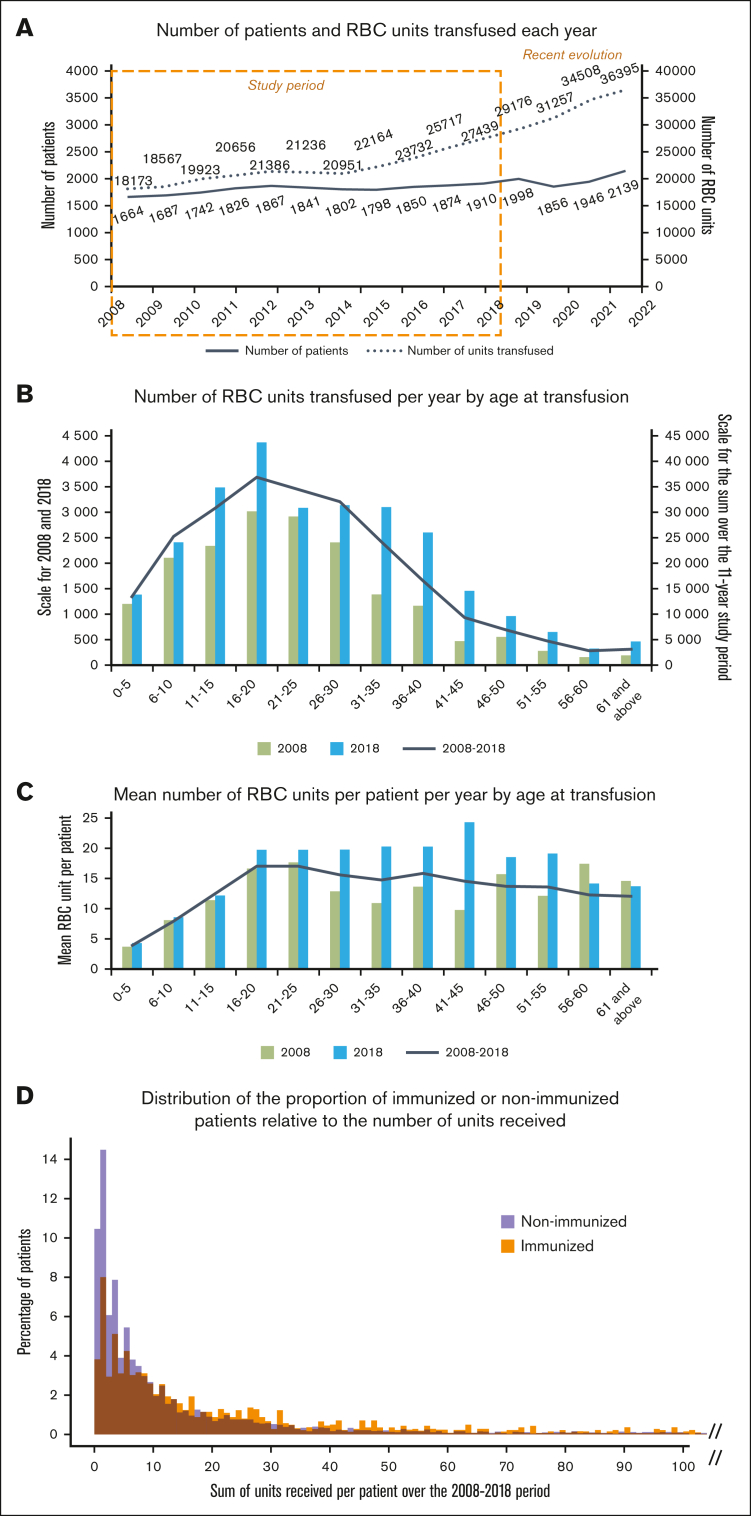
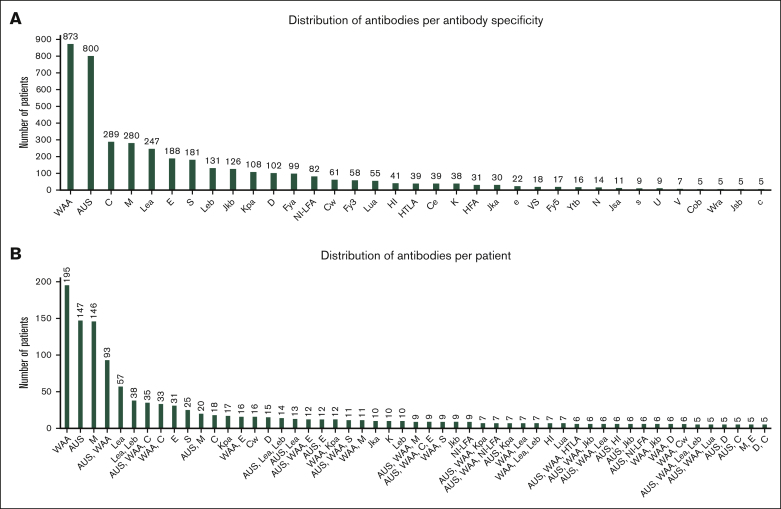
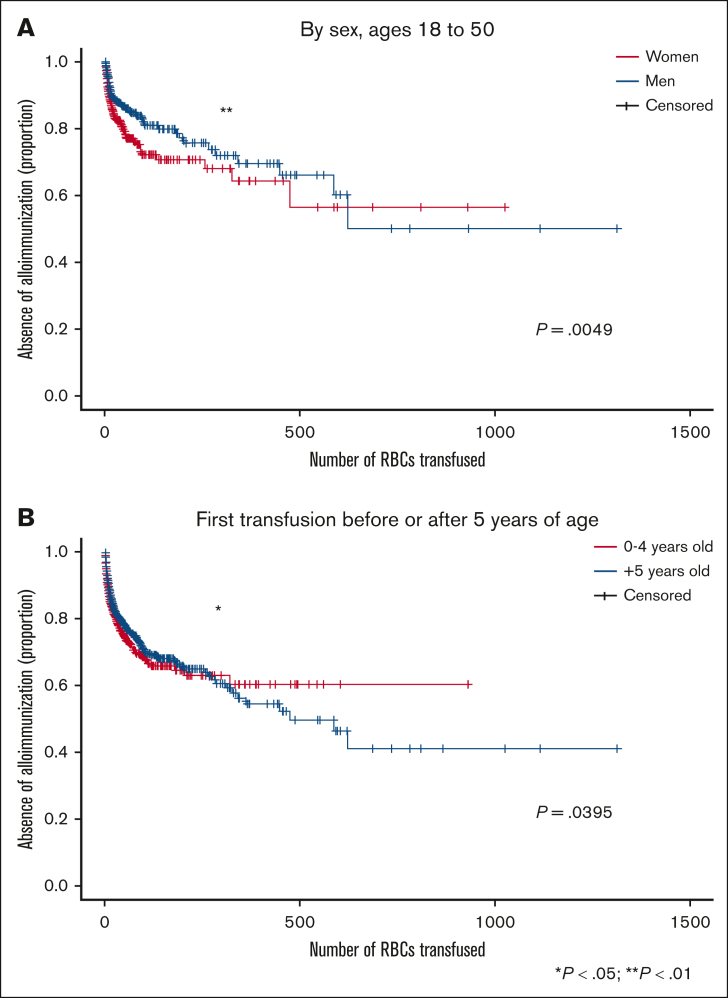
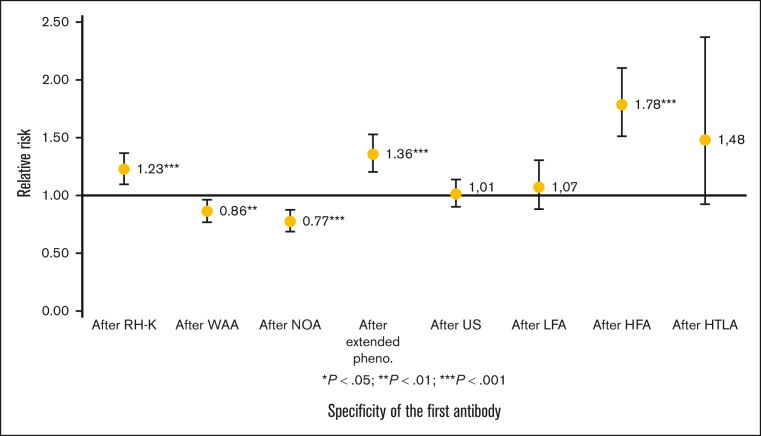
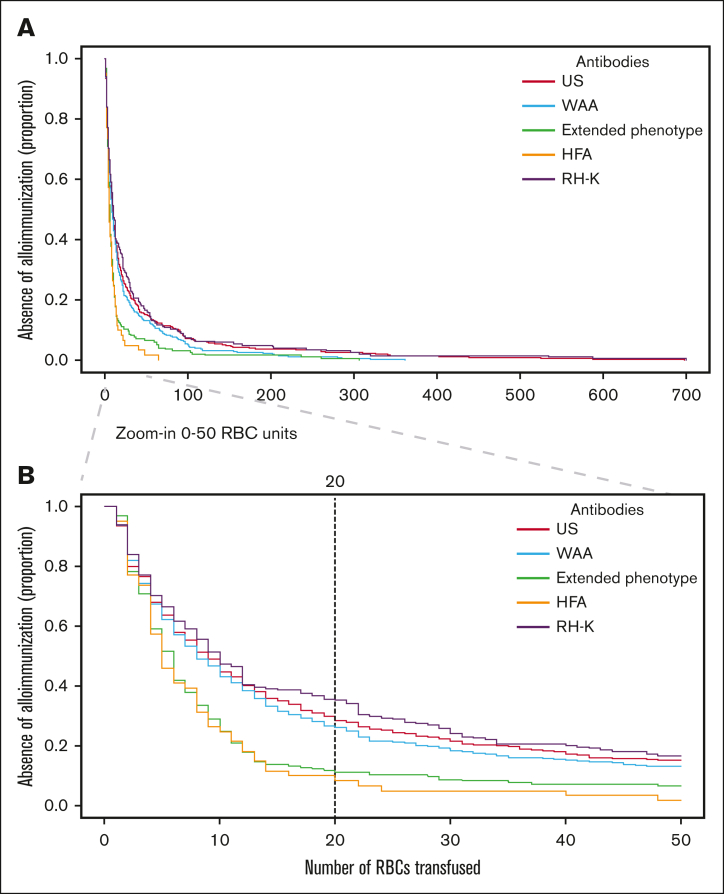
Red blood cell (RBC) transfusion is a major therapy for sickle cell disease (SCD). Patients are at risk of forming antibodies to RBC antigens, which can result in the impossibility to find compatible units and can cause hemolytic transfusion reactions. This retrospective study investigates the evolution of RBC consumption and the frequencies, specificities, and chronology of the appearance of antibodies in a population of patients consistently receiving RH (C, D, E, c, e) and K-matched RBC units (RBCus) from a predominantly European donor population. Over the 11-year period in the Paris area, 6496 patients received transfusion at least once for a total of 239 944 units. Antibodies were made by 1742 patients. The first antibodies of a patient were predictive of subsequent immunization. By the 17th RBCu transfused (by the 20th, excluding warm autoantibodies), 75% of the patients who would make antibodies had made their first. By the 16th, 90% who would make antibodies to a high frequency antigen had made their first antibody to these antigens. Females made their first antibodies slightly earlier than males. Patients who received multiple transfusions (>50 units) had a higher immunization prevalence than those who rarely received transfusion (<12 units) but fewer clinically significant antibodies. Patients with SCD and prophylactic RH-K matching not immunized by the 20th RBCu are likely to have a low alloimmunization risk (to antigens other than RH-K), that is, be low responders, especially relative to the most clinically significant antibodies. This number of 20 units is a point before which close monitoring of patients is most important but remains open to future adjustment.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Vichinsky EP, Earles A, Johnson RA, Hoag MS, Williams A, Lubin B. Alloimmunization in sickle cell anemia and transfusion of racially unmatched blood. N Engl J Med. 1990;322(23):1617–1621. - PubMed
-
- Natukunda B, Schonewille H, van de Watering L, Brand A. Prevalence and specificities of red blood cell alloantibodies in transfused Ugandans with different diseases. Vox Sang. 2010;98(2):167–171. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
