

Clinical and molecular characteristics of early-onset vs average-onset esophagogastric cancer
- PMID: 37699004
- PMCID: PMC10852615
- DOI: 10.1093/jnci/djad186
Clinical and molecular characteristics of early-onset vs average-onset esophagogastric cancer
Abstract
Background: The rate of esophagogastric cancer is rising among individuals under 50 years of age. It remains unknown whether early-onset esophagogastric cancer represents a unique entity. This study investigated the clinical and molecular characteristics of early-onset and average-onset esophagogastric cancer .
Methods: We reviewed the Memorial Sloan Kettering Cancer Center gastric, esophageal, and gastroesophageal junction cancer database. Associations between baseline characteristics and tumor and germline molecular alterations were compared between those with early-onset and average-onset esophagogastric cancer using Fisher exact tests and the Benjamini-Hochberg method for multiple-hypothesis correction.
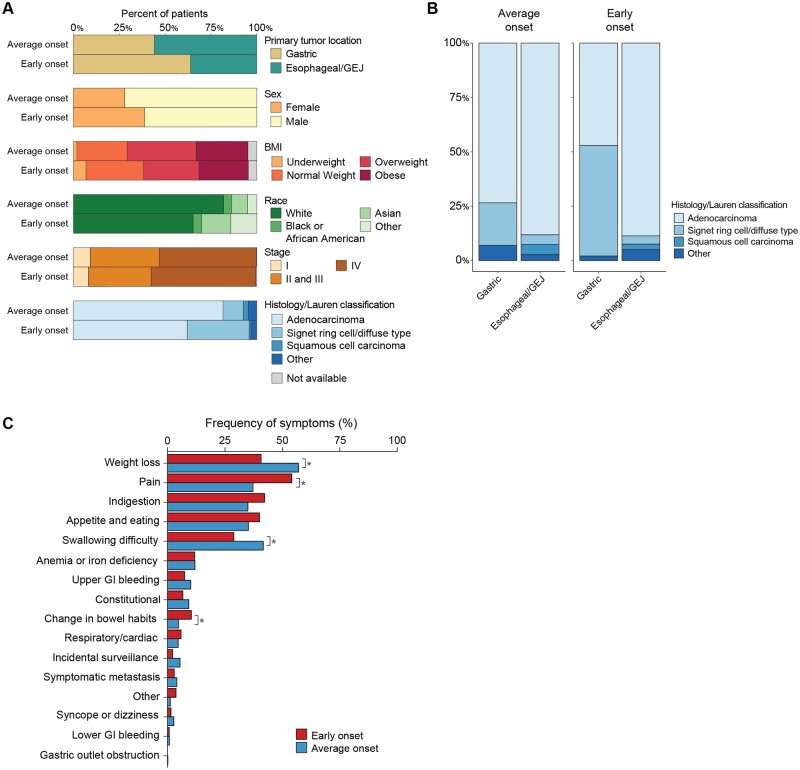
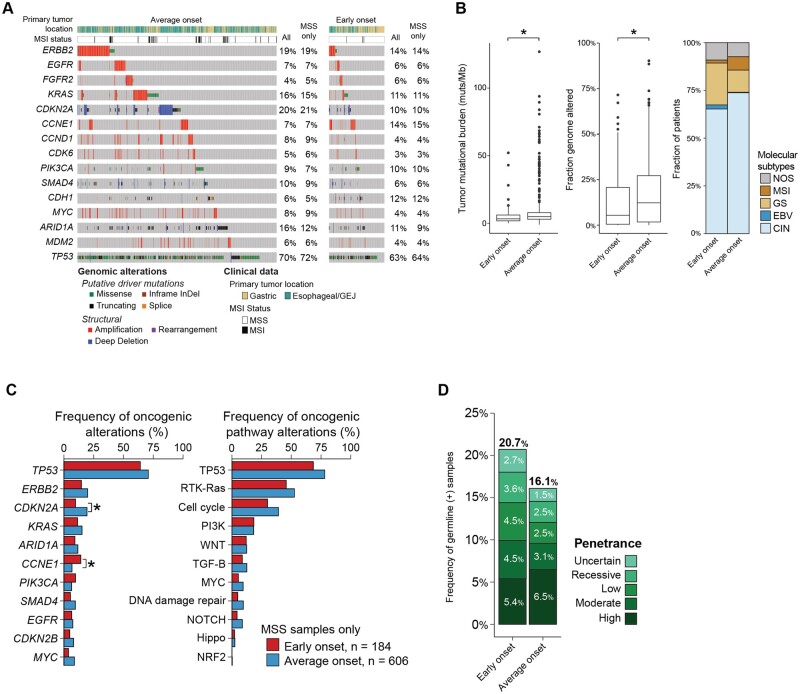
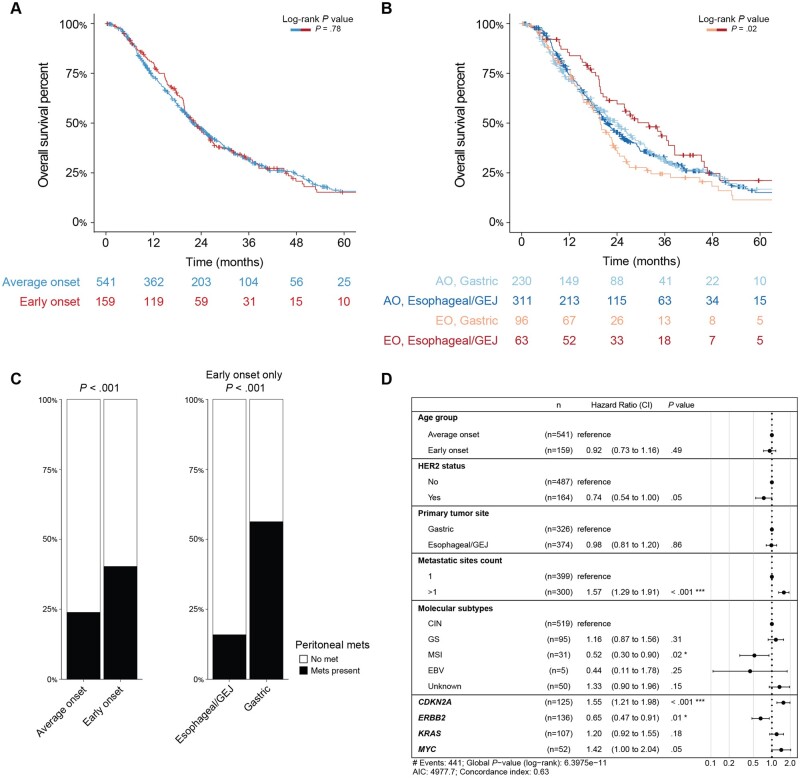
Results: We included 1123 patients with early-onset esophagogastric cancer (n = 219; median age = 43 years [range = 18-49 years]) and average-onset esophagogastric cancer (n = 904; median age = 67 years [range = 50-94 years]) treated between 2005 and 2018. The early-onset group had more women (39% vs 28%, P = .002). Patients with early-onset esophagogastric cancer were more likely to have a gastric primary site (64% vs 44%, P < .0001). The signet ring cell and/or diffuse type was 3 times more common in the early-onset esophagogastric cancer group (31% vs 9%, P < .0001). Early-onsite tumors were more frequently genomically stable (31% vs 18%, P = .0002) and unlikely to be microsatellite instability high (2% vs 7%, P = .003). After restricting to adenocarcinoma and signet ring cell and/or diffuse type carcinomas, we observed no difference in stage (P = .40) or overall survival from stage IV diagnosis (median = 22.7 vs 22.1 months, P = .78).
Conclusions: Our study supported a preponderance of gastric primary disease sites, signet ring histology, and genomically stable molecular subtypes in early-onset esophagogastric cancer. Our findings highlight the need for further research to define the underlying pathogenesis and strategies for early detection and prevention.
© The Author(s) 2023. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
G.Y.K. provides services for AstraZeneca, Bristol-Myers Squibb, Merck & Co Inc, and Zymeworks Inc. D.H.I. provides services for Amgen, Astellas, Bayer, Bristol Myers Squibb, Daiichi Sankyo, Lilly Oncology, MacroGenics, Inc, Merck & Co Inc, Natera Inc, Roche, and Taiho. N.S. provides services for Cambridge Innovation Institute, Harvard T. H. Chan School of Public Health, Innovation in Cancer Informatics, and Seoul National University. Y.Y.J. has received research funding from Bayer, Bristol Myers Squibb, Cycle for Survival, the US Department of Defense, Eli Lilly, Fred’s Team, Genentech/Roche, Merck, the National Cancer Institute, and RGENIX and has served on advisory boards or in a consulting role for Amerisource Bergen, Arcus Biosciences, Astra Zeneca, Basilea Pharmaceutica, Bayer, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly, Geneos Therapeutics, GlaxoSmithKline, Imedex, Imugene, Lynx Health, Merck, Merck Serono, Michael J. Hennessy Associates, Paradigm Medical Communications, PeerView Institute, Pfizer, Research to Practice, RGENIX, Seagen, Silverback Therapeutics, and Zymeworks Inc. A.C. has consulting or advisory roles with Bayer, GlaxoSmithKline, Incyyte, Merck, Janssen, Seattle Genetics, and G1 Therapeutics and research funding from Seattle Genetics, Rgenix (Inst), and GlaxoSmithKline.
M.A.L., H.W., W.C., Y.K., A.M., E.W., J.L., S.S.J., P.G., M.A.S., M.L., H.G., D.R.J, S.S., D.G.C., L.H.T., V.E.S., D.M., and Z.K.S. have no relevant financial relationships to disclose. No other potential conflicts of interest relevant to this article exist.
Figures
References
-
- Howlader N, Noone AM, Krapcho M, et al. Cancer Statistics Review, 1975-2017 - SEER Statistics. SEER Cancer Statistics Review, 1975-2017. Bethesda, MD: National Cancer Institute; 2019. https://seer.cancer.gov/csr/1975_2017/.
-
- Islami F, DeSantis CE, Jemal A.. Incidence trends of esophageal and gastric cancer subtypes by race, ethnicity, and age in the United States, 1997–2014. Clin Gastroenterol Hepatol. 2019;17(3):429-439. - PubMed
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. - PubMed
-
- Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941-1953. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
