

Aggressive surgical approach with vascular resection and reconstruction for retroperitoneal sarcomas: a systematic review
- PMID: 37700246
- PMCID: PMC10498574
- DOI: 10.1186/s12893-023-02178-1
Aggressive surgical approach with vascular resection and reconstruction for retroperitoneal sarcomas: a systematic review
Abstract
Background and aim: Surgery is the mainstay of treatment and completeness of surgical resection is critical to achieve local control for retroperitoneal sarcoma (RPS). En-bloc resection of adjacent organs, including major abdominal vessels, is often required to achieve negative margins. The aim of this review was to summarise the available evidence to assess the relative benefits and disadvantages of an aggressive surgical approach with vascular resection in patients with retroperitoneal sarcoma (RPS).
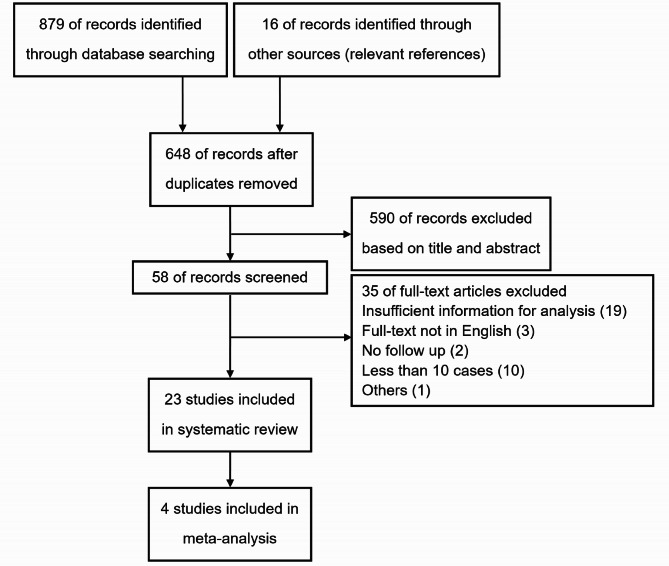
Methods: We searched PubMed, the Cochrane Library, and EMBASE for relevant studies published from inception up to August 1, 2022. We performed a systematic review of the available studies to assess the safety and long-term survival results of vascular resection for RPS.
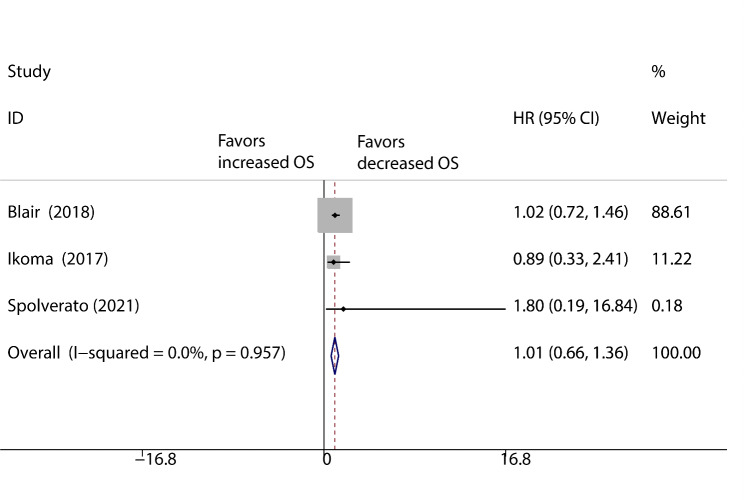
Results: We identified a total of 23 studies for our review. Overall postoperative in-hospital or 30-day mortality rate of patients with primary iliocaval leiomyosarcoma was 3% (11/359), and the major complication rate was 13%. The recurrence-free survival (RFS) rates after the follow-up period varied between 15% and 52%, and the 5-year overall survival (OS) rates ranged from 25 to 78%. Overall postoperative in-hospital or 30-day mortality rate of patients with RPSs receiving vascular resection was 3%, and the major complication rate was 27%. The RFS rates after the follow-up period were 18-86%, and the 5-year OS rates varied between 50% and 73%. There were no significant differences in the rates of RFS (HR: 0.97; 95% CI: 0.74-1.19; p = 0.945) and OS (HR: 1.01; 95% CI: 0.66-1.36; p = 0.774) between the extended resection group and tumour resection alone group.
Conclusions: With adequate preparation and proper management, for patients with RPSs involving major vessels, aggressive surgical approach with vascular resection can achieve R0/R1 resection and improve survival.
Keywords: Overall survival; Retroperitoneal sarcoma; Surgery; Systematic review; Vascular resection.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Survival outcomes of surgery for retroperitoneal sarcomas: A systematic review and meta-analysis.PLoS One. 2022 Jul 28;17(7):e0272044. doi: 10.1371/journal.pone.0272044. eCollection 2022. PLoS One. 2022. PMID: 35901187 Free PMC article.
-
Aggressive surgical approach with major vascular resection for retroperitoneal sarcomas.PLoS One. 2025 Mar 20;20(3):e0320066. doi: 10.1371/journal.pone.0320066. eCollection 2025. PLoS One. 2025. PMID: 40111953 Free PMC article.
-
Analysis of outcomes and predictors of long-term survival following resection for retroperitoneal sarcoma.BMC Surg. 2019 Jun 10;19(1):61. doi: 10.1186/s12893-019-0521-9. BMC Surg. 2019. PMID: 31182086 Free PMC article.
-
Retroperitoneal sarcoma: 25 years of experience with aggressive surgical treatment at the Institute of Oncology, Ljubljana.J Surg Oncol. 2005 Jul 1;91(1):1-9. doi: 10.1002/jso.20265. J Surg Oncol. 2005. PMID: 15999353
-
[Systematic surgery of retroperitoneal sarcomas : Imaging-guided planning of surgical strategy].Chirurg. 2019 Jun;90(6):447-456. doi: 10.1007/s00104-019-0952-y. Chirurg. 2019. PMID: 31001643 Review. German.
Cited by
-
3D-SARC: A Pilot Study Testing the Use of a 3D Augmented-Reality Model with Conventional Imaging as a Preoperative Assessment Tool for Surgical Resection of Retroperitoneal Sarcoma.Ann Surg Oncol. 2024 Oct;31(10):7198-7205. doi: 10.1245/s10434-024-15634-w. Epub 2024 Jun 19. Ann Surg Oncol. 2024. PMID: 38898325
-
Patient Experiences After Aborted Cancer Surgery: A Qualitative Study.Ann Surg Oncol. 2023 Oct;30(11):6844-6851. doi: 10.1245/s10434-023-14046-6. Epub 2023 Aug 4. Ann Surg Oncol. 2023. PMID: 37540329
-
Unresectable leiomyosarcoma of the inferior vena cava with right atrium tumor thrombus: when to deem this tumor inoperable? A case report and literature review.Front Oncol. 2024 Jan 4;13:1331896. doi: 10.3389/fonc.2023.1331896. eCollection 2023. Front Oncol. 2024. PMID: 38282675 Free PMC article.
-
Surgical outcomes of major vascular resection for retroperitoneal liposarcoma from a high‑volume sarcoma center: a propensity score matching analysis.J Cancer Res Clin Oncol. 2024 Jul 9;150(7):343. doi: 10.1007/s00432-024-05871-7. J Cancer Res Clin Oncol. 2024. PMID: 38981922 Free PMC article.
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. - PubMed
-
- Porter GA, Baxter NN, Pisters PW. Retroperitoneal sarcoma: a population-based analysis of epidemiology, surgery, and radiotherapy. Cancer. 2006;106(7):1610–6. - PubMed
-
- Dingley B, Fiore M, Gronchi A. Personalizing surgical margins in retroperitoneal sarcomas: an update. Expert Rev Anticancer Ther. 2019;19(7):613–31. - PubMed
-
- Bonvalot S, Gronchi A, Le Péchoux C, Swallow CJ, Strauss D, Meeus P, et al. Preoperative radiotherapy plus surgery versus surgery alone for patients with primary retroperitoneal sarcoma (EORTC-62092: STRASS): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2020;21(10):1366–77. - PubMed
-
- Fairweather M, Gonzalez RJ, Strauss D, Raut CP. Current principles of surgery for retroperitoneal sarcomas. J Surg Oncol. 2018;117(1):33–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
