

Prevention of cardiac surgery-associated acute kidney injury: a systematic review and meta-analysis of non-pharmacological interventions
- PMID: 37700297
- PMCID: PMC10498585
- DOI: 10.1186/s13054-023-04640-1
Prevention of cardiac surgery-associated acute kidney injury: a systematic review and meta-analysis of non-pharmacological interventions
Abstract
Background: Cardiac surgery-associated acute kidney injury (CSA-AKI) is frequent. While two network meta-analyses assessed the impact of pharmacological interventions to prevent CSA-AKI, none focused on non-pharmacological interventions. We aim to assess the effectiveness of non-pharmacological interventions to reduce the incidence of CSA-AKI.
Methods: We searched PubMed, Embase, Central and clinical trial registries from January 1, 2004 (first consensus definition of AKI) to July 1, 2023. Additionally, we conducted manual screening of abstracts of major anesthesia and intensive care conferences over the last 5 years and reference lists of relevant studies. We selected all randomized controlled trials (RCTs) assessing a non-pharmacological intervention to reduce the incidence of CSA-AKI, without language restriction. We excluded RCTs of heart transplantation or involving a pediatric population. The primary outcome variable was CSA-AKI. Two reviewers independently identified trials, extracted data and assessed risk of bias. Random-effects meta-analyses were conducted to calculate risk ratios (RRs) with 95% confidence intervals (CIs). We used the Grading of Recommendations Assessment, Development, and Evaluation to assess the quality of evidence.
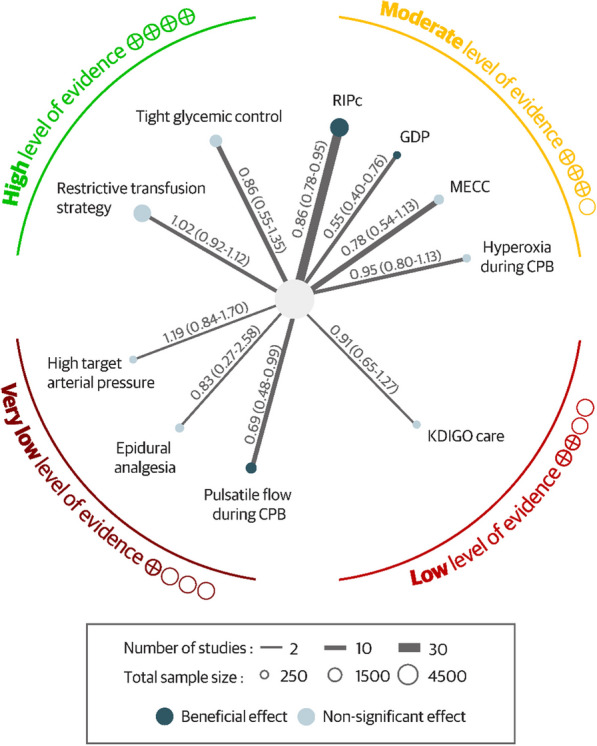
Results: We included 86 trials (25,855 patients) evaluating 10 non-pharmacological interventions to reduce the incidence of CSA-AKI. No intervention had high-quality evidence to reduce CSA-AKI. Two interventions were associated with a significant reduction in CSA-AKI incidence, with moderate quality of evidence: goal-directed perfusion (RR, 0.55 [95% CI 0.40-0.76], I2 = 0%; Phet = 0.44) and remote ischemic preconditioning (RR, 0.86 [0.78-0.95]; I2 = 23%; Phet = 0.07). Pulsatile flow during cardiopulmonary bypass was associated with a significant reduction in CSA-AKI incidence but with very low quality of evidence (RR = 0.69 [0.48; 0.99]; I2 = 53%; Phet < 0.01). We found high quality of evidence for lack of effect of restrictive transfusion strategy (RR, 1.02 [95% CI 0.92; 1.12; Phet = 0.67; I2 = 3%) and tight glycemic control (RR, 0.86 [95% CI 0.55; 1.35]; Phet = 0.25; I2 = 26%).
Conclusions: Two non-pharmacological interventions are likely to reduce CSA-AKI incidence, with moderate quality of evidence: goal-directed perfusion and remote ischemic preconditioning.
Keywords: Acute kidney injury; Cardiac surgery; Non-pharmacological interventions; Prevention.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures



References
-
- Hoste EA, Cruz DN, Davenport A, Mehta RL, Piccinni P, Tetta C, et al. The epidemiology of cardiac surgery-associated acute kidney injury. Int J Artif Organs. 2008;31:158–165. - PubMed
-
- Karkouti K, Wijeysundera DN, Yau TM, Callum JL, Cheng DC, Crowther M, et al. Acute kidney injury after cardiac surgery: focus on modifiable risk factors. Circulation. 2009;119:495–502. - PubMed
-
- Lopez-Delgado JC, Esteve F, Torrado H, Rodríguez-Castro D, Carrio ML, Farrero E, et al. Influence of acute kidney injury on short- and long-term outcomes in patients undergoing cardiac surgery: risk factors and prognostic value of a modified RIFLE classification. Crit Care. 2013;17:R293. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
