

Impact of measurement and feedback on chlorhexidine gluconate bathing among intensive care unit patients: A multicenter study
- PMID: 37700540
- PMCID: PMC10859163
- DOI: 10.1017/ice.2023.177
Impact of measurement and feedback on chlorhexidine gluconate bathing among intensive care unit patients: A multicenter study
Abstract
Objective: To assess whether measurement and feedback of chlorhexidine gluconate (CHG) skin concentrations can improve CHG bathing practice across multiple intensive care units (ICUs).
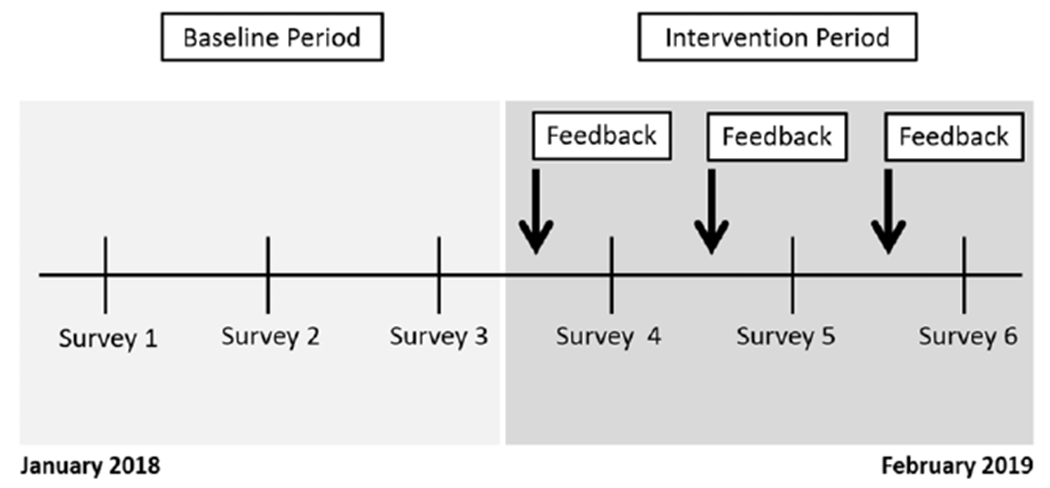
Design: A before-and-after quality improvement study measuring patient CHG skin concentrations during 6 point-prevalence surveys (3 surveys each during baseline and intervention periods).
Setting: The study was conducted across 7 geographically diverse ICUs with routine CHG bathing.
Participants: Adult patients in the medical ICU.
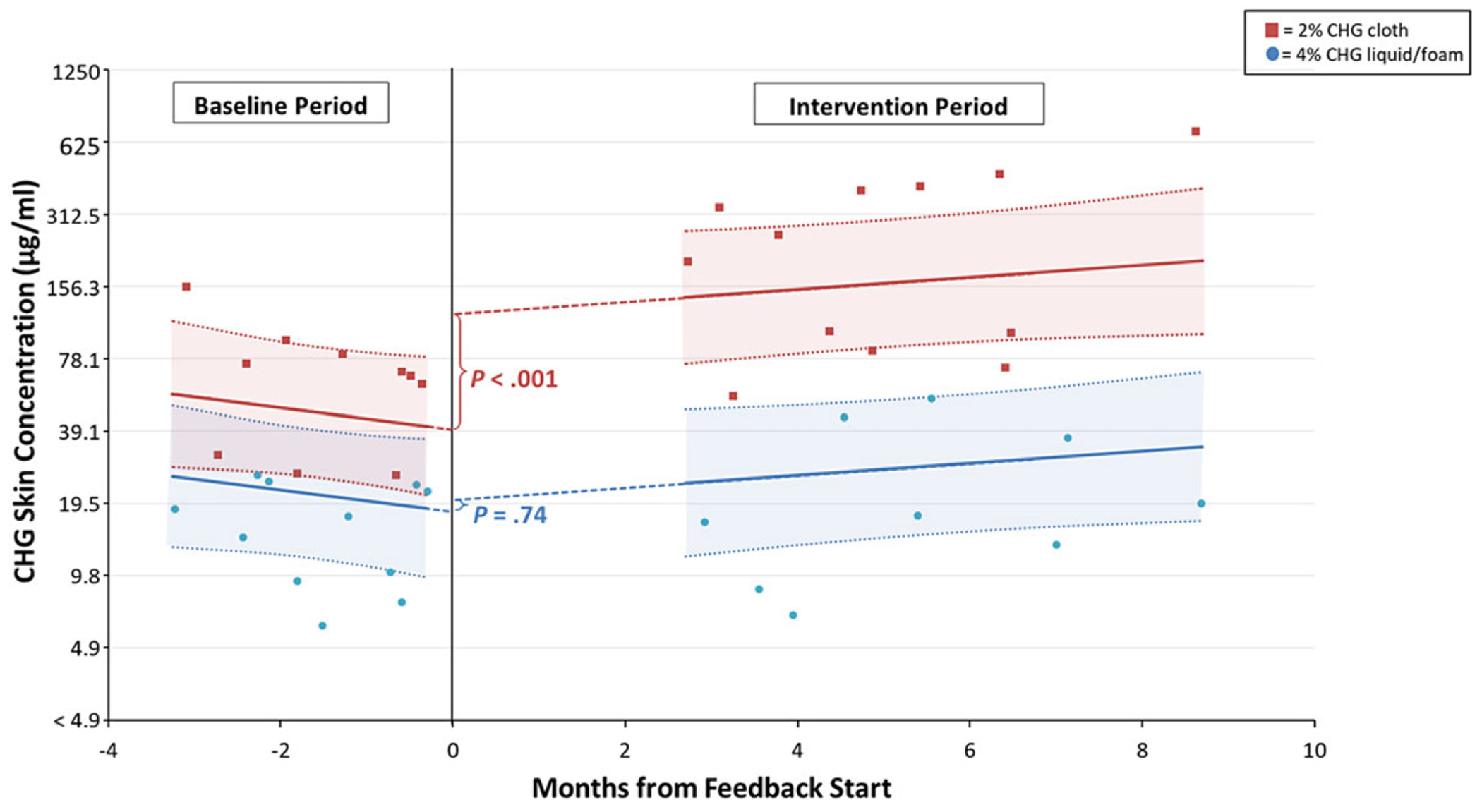
Methods: CHG skin concentrations were measured at the neck, axilla, and inguinal region using a semiquantitative colorimetric assay. Aggregate unit-level CHG skin concentration measurements from the baseline period and each intervention period survey were reported back to ICU leadership, which then used routine education and quality improvement activities to improve CHG bathing practice. We used multilevel linear models to assess the impact of intervention on CHG skin concentrations.
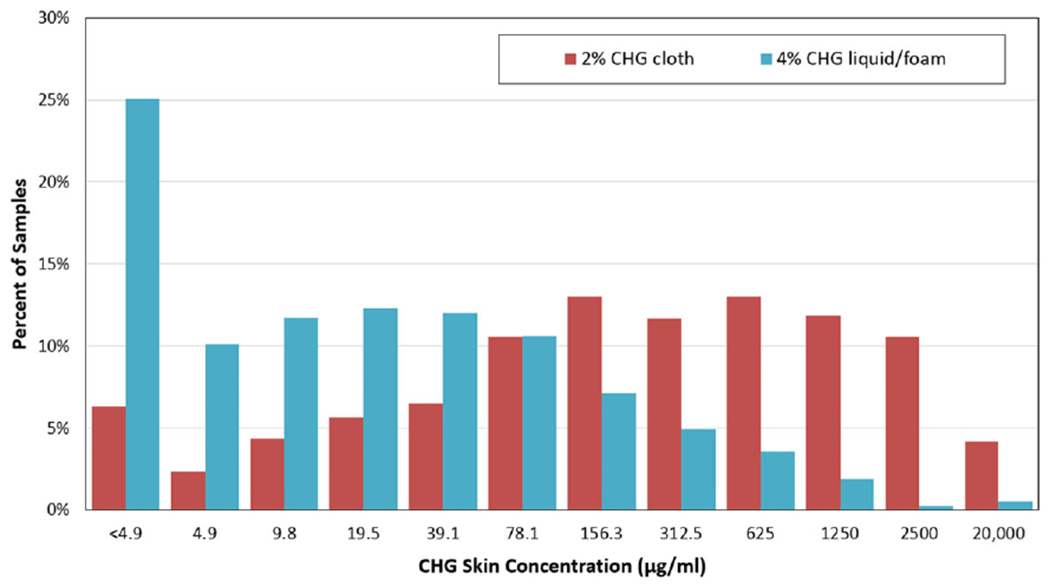
Results: We enrolled 681 (93%) of 736 eligible patients; 92% received a CHG bath prior to survey. At baseline, CHG skin concentrations were lowest on the neck, compared to axillary or inguinal regions (P < .001). CHG was not detected on 33% of necks, 19% of axillae, and 18% of inguinal regions (P < .001 for differences in body sites). During the intervention period, ICUs that used CHG-impregnated cloths had a 3-fold increase in patient CHG skin concentrations as compared to baseline (P < .001).
Conclusions: Routine CHG bathing performance in the ICU varied across multiple hospitals. Measurement and feedback of CHG skin concentrations can be an important tool to improve CHG bathing practice.
Conflict of interest statement
M.K.H. has been a coinvestigator on several research studies for which Sage Products (now part of Stryker Corporation), Molnlycke, and Medline provided chlorhexidine products at no charge to hospitals and skilled nursing facilities participating in the research. Neither M.K.H. nor her employer (Rush University Medical Center) received chlorhexidine products. S.G. is a coinvestigator on a study in which participating hospital and nursing homes received contributed antiseptic product from Stryker (Sage Pharmaceuticals), Clorox, Medline, and Xttrium; companies had no role in the design, conduct, analysis, or publication of these studies. C.R. reports royalties from UpToDate, Inc, and consulting fees from Pfizer and Cytovale for topics unrelated to this study. D.W. was a consultant for Molynlycke Health Care AB after completion of the study. M.Y.L. has received research support in the form of contributed product from Sage Products (now part of Stryker Corporation).
Figures
Similar articles
-
Chlorhexidine gluconate bathing practices and skin concentrations in intensive care unit patients.Am J Infect Control. 2018 Feb;46(2):226-228. doi: 10.1016/j.ajic.2017.08.022. Epub 2017 Oct 6. Am J Infect Control. 2018. PMID: 28993110
-
Implementing daily chlorhexidine gluconate treatment for the prevention of healthcare-associated infections in non-intensive care settings: A multiple case analysis.PLoS One. 2020 Apr 24;15(4):e0232062. doi: 10.1371/journal.pone.0232062. eCollection 2020. PLoS One. 2020. PMID: 32330165 Free PMC article.
-
A Multicenter Pragmatic Interrupted Time Series Analysis of Chlorhexidine Gluconate Bathing in Community Hospital Intensive Care Units.Infect Control Hosp Epidemiol. 2016 Jul;37(7):791-7. doi: 10.1017/ice.2016.23. Epub 2016 Feb 10. Infect Control Hosp Epidemiol. 2016. PMID: 26861417 Free PMC article. Clinical Trial.
-
A Quality Improvement Project to Decrease CLABSIs in Non-ICU Settings.Qual Manag Health Care. 2023 Jul-Sep 01;32(3):189-196. doi: 10.1097/QMH.0000000000000375. Epub 2022 Nov 5. Qual Manag Health Care. 2023. PMID: 36346987 Review.
-
Evidence for the effectiveness of chlorhexidine bathing and health care-associated infections among adult intensive care patients: a trial sequential meta-analysis.BMC Infect Dis. 2018 Dec 19;18(1):679. doi: 10.1186/s12879-018-3521-y. BMC Infect Dis. 2018. PMID: 30567493 Free PMC article. Review.
Cited by
-
Rapid Environmental Contamination With Candida auris and Multidrug-Resistant Bacterial Pathogens Near Colonized Patients.Clin Infect Dis. 2024 May 15;78(5):1276-1284. doi: 10.1093/cid/ciad752. Clin Infect Dis. 2024. PMID: 38059527 Free PMC article.
-
Can chlorhexidine gluconate baths reduce fungal colonisation in intensive care unit patients?Antimicrob Resist Infect Control. 2025 Jul 9;14(1):87. doi: 10.1186/s13756-025-01606-6. Antimicrob Resist Infect Control. 2025. PMID: 40635094 Free PMC article.
-
Relationship between chlorhexidine gluconate concentration and microbial colonization of patients' skin.Infect Control Hosp Epidemiol. 2024 May 28:1-6. doi: 10.1017/ice.2024.81. Online ahead of print. Infect Control Hosp Epidemiol. 2024. PMID: 38804007
References
-
- Bleasdale SC, Trick WE, Gonzalez IM, Lyles RD, Hayden MK, Weinstein RA. Effectiveness of chlorhexidine bathing to reduce catheter-associated bloodstream infections in medical intensive care unit patients. Arch Intern Med 2007;167:2073–2079. - PubMed
-
- Supple L, Kumaraswami M, Kundrapu S, et al. Chlorhexidine only works if applied correctly: use of a simple colorimetric assay to provide monitoring and feedback on effectiveness of chlorhexidine application. Infect Control Hosp Epidemiol 2015;36:1095–1097. - PubMed
