

Higher versus lower fractions of inspired oxygen or targets of arterial oxygenation for adults admitted to the intensive care unit
- PMID: 37700687
- PMCID: PMC10498149
- DOI: 10.1002/14651858.CD012631.pub3
Higher versus lower fractions of inspired oxygen or targets of arterial oxygenation for adults admitted to the intensive care unit
Abstract
Background: This is an updated review concerning 'Higher versus lower fractions of inspired oxygen or targets of arterial oxygenation for adults admitted to the intensive care unit'. Supplementary oxygen is provided to most patients in intensive care units (ICUs) to prevent global and organ hypoxia (inadequate oxygen levels). Oxygen has been administered liberally, resulting in high proportions of patients with hyperoxemia (exposure of tissues to abnormally high concentrations of oxygen). This has been associated with increased mortality and morbidity in some settings, but not in others. Thus far, only limited data have been available to inform clinical practice guidelines, and the optimum oxygenation target for ICU patients is uncertain. Because of the publication of new trial evidence, we have updated this review.
Objectives: To update the assessment of benefits and harms of higher versus lower fractions of inspired oxygen (FiO2) or targets of arterial oxygenation for adults admitted to the ICU.
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, Science Citation Index Expanded, BIOSIS Previews, and LILACS. We searched for ongoing or unpublished trials in clinical trial registers and scanned the reference lists and citations of included trials. Literature searches for this updated review were conducted in November 2022.
Selection criteria: We included randomised controlled trials (RCTs) that compared higher versus lower FiO2 or targets of arterial oxygenation (partial pressure of oxygen (PaO2), peripheral or arterial oxygen saturation (SpO2 or SaO2)) for adults admitted to the ICU. We included trials irrespective of publication type, publication status, and language. We excluded trials randomising participants to hypoxaemia (FiO2 below 0.21, SaO2/SpO2 below 80%, or PaO2 below 6 kPa) or to hyperbaric oxygen, and cross-over trials and quasi-randomised trials.
Data collection and analysis: Four review authors independently, and in pairs, screened the references identified in the literature searches and extracted the data. Our primary outcomes were all-cause mortality, the proportion of participants with one or more serious adverse events (SAEs), and quality of life. We analysed all outcomes at maximum follow-up. Only three trials reported the proportion of participants with one or more SAEs as a composite outcome. However, most trials reported on events categorised as SAEs according to the International Conference on Harmonisation Good Clinical Practice (ICH-GCP) criteria. We, therefore, conducted two analyses of the effect of higher versus lower oxygenation strategies using 1) the single SAE with the highest reported proportion in each trial, and 2) the cumulated proportion of participants with an SAE in each trial. Two trials reported on quality of life. Secondary outcomes were lung injury, myocardial infarction, stroke, and sepsis. No trial reported on lung injury as a composite outcome, but four trials reported on the occurrence of acute respiratory distress syndrome (ARDS) and five on pneumonia. We, therefore, conducted two analyses of the effect of higher versus lower oxygenation strategies using 1) the single lung injury event with the highest reported proportion in each trial, and 2) the cumulated proportion of participants with ARDS or pneumonia in each trial. We assessed the risk of systematic errors by evaluating the risk of bias in the included trials using the Risk of Bias 2 tool. We used the GRADEpro tool to assess the overall certainty of the evidence. We also evaluated the risk of publication bias for outcomes reported by 10b or more trials.
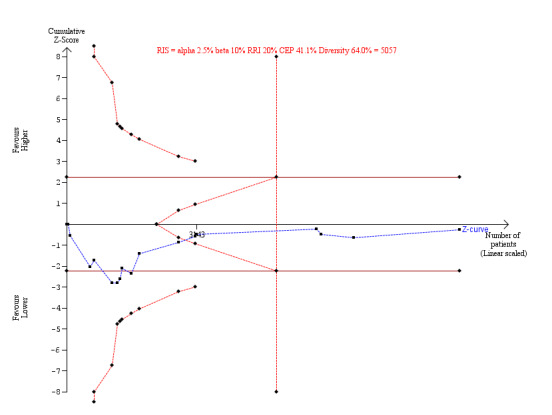
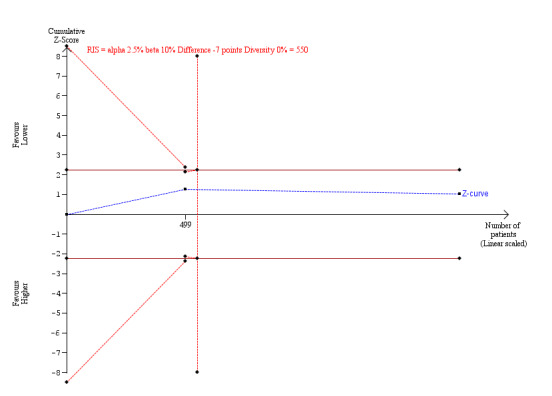
Main results: We included 19 RCTs (10,385 participants), of which 17 reported relevant outcomes for this review (10,248 participants). For all-cause mortality, 10 trials were judged to be at overall low risk of bias, and six at overall high risk of bias. For the reported SAEs, 10 trials were judged to be at overall low risk of bias, and seven at overall high risk of bias. Two trials reported on quality of life, of which one was judged to be at overall low risk of bias and one at high risk of bias for this outcome. Meta-analysis of all trials, regardless of risk of bias, indicated no significant difference from higher or lower oxygenation strategies at maximum follow-up with regard to mortality (risk ratio (RR) 1.01, 95% confidence interval (C)I 0.96 to 1.06; I2 = 14%; 16 trials; 9408 participants; very low-certainty evidence); occurrence of SAEs: the highest proportion of any specific SAE in each trial RR 1.01 (95% CI 0.96 to 1.06; I2 = 36%; 9466 participants; 17 trials; very low-certainty evidence), or quality of life (mean difference (MD) 0.5 points in participants assigned to higher oxygenation strategies (95% CI -2.75 to 1.75; I2 = 34%, 1649 participants; 2 trials; very low-certainty evidence)). Meta-analysis of the cumulated number of SAEs suggested benefit of a lower oxygenation strategy (RR 1.04 (95% CI 1.02 to 1.07; I2 = 74%; 9489 participants; 17 trials; very low certainty evidence)). However, trial sequential analyses, with correction for sparse data and repetitive testing, could reject a relative risk increase or reduction of 10% for mortality and the highest proportion of SAEs, and 20% for both the cumulated number of SAEs and quality of life. Given the very low-certainty of evidence, it is necessary to interpret these findings with caution. Meta-analysis of all trials indicated no statistically significant evidence of a difference between higher or lower oxygenation strategies on the occurrence of lung injuries at maximum follow-up (the highest reported proportion of lung injury RR 1.08, 95% CI 0.85 to 1.38; I2 = 0%; 2048 participants; 8 trials; very low-certainty evidence). Meta-analysis of all trials indicated harm from higher oxygenation strategies as compared with lower on the occurrence of sepsis at maximum follow-up (RR 1.85, 95% CI 1.17 to 2.93; I2 = 0%; 752 participants; 3 trials; very low-certainty evidence). Meta-analysis indicated no differences regarding the occurrences of myocardial infarction or stroke.
Authors' conclusions: In adult ICU patients, it is still not possible to draw clear conclusions about the effects of higher versus lower oxygenation strategies on all-cause mortality, SAEs, quality of life, lung injuries, myocardial infarction, stroke, and sepsis at maximum follow-up. This is due to low or very low-certainty evidence.
Trial registration: ClinicalTrials.gov NCT02321072.
Copyright © 2023 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
Thomas Lass Klitgaard: Co‐ordinating investigator of the Handling Oxygenation Targets in the Intensive Care Unit (HOT‐ICU) trial, a randomised clinical trial comparing a higher versus lower oxygenation target in adult patients with hypoxaemic respiratory failure acutely admitted to the intensive care unit. Also, co‐ordinating investigator of the Handling Oxygenation Targets in COVID‐19 (HOT‐COVID) trial, a randomised clinical trial comparing a higher versus lower oxygenation target in adult patients with COVID‐19 and hypoxaemic respiratory failure acutely admitted to the intensive care unit.
Olav Lilleholt Schjørring: Olav's Ph.D. study was funded through a grant from the Innovation Fund Denmark. Furthermore, he was the co‐ordinating investigator of the Handling Oxygenation Targets in the Intensive Care Unit (HOT‐ICU) trial, a randomised clinical trial comparing a higher versus lower oxygenation target in adult patients with hypoxaemic respiratory failure acutely admitted to the intensive care unit.
Frederik Mølgaard Nielsen: Co‐ordinating investigator of the Handling Oxygenation Targets in COVID‐19 (HOT‐COVID) trial, a randomised clinical trial comparing a higher versus lower oxygenation target in adult patients with COVID‐19 and hypoxaemic respiratory failure acutely admitted to the intensive care unit.
Christian Sylvest Meyhoff: Chief investigator for the VitamIn and oXygen Interventions and Cardiovascular Events (VIXIE) trial (a randomised controlled trial comparing perioperative oxygen fractions); site investigator in the HOT‐ICU trial (a randomised controlled trial investigating oxygenation targets in the intensive care unit); co‐author of several Cochrane Reviews about oxygen therapy; and was the primary investigator of the PROXI trial (a randomised controlled trial comparing perioperative oxygen fractions).
Anders Perner: Anders's institution receives money for research from Ferring Pharmaceuticals and the Novo Nordisk Foundation
Jørn Wetterslev: Jørn is a member of the task force on Trial Sequential Analysis (TSA) at the Copenhagen Trial Unit, developing and programming TSA (see
Bodil Steen Rasmussen: Bodil is the sponsor and primary investigator of a randomised clinical trial comparing a higher versus lower oxygenation target in adult patients with hypoxaemic respiratory failure acutely admitted to the intensive care unit (the Handling Oxygenation Targets in the Intensive Care Unit (HOT‐ICU) trial (NCT03174002)). Bodil is also sponsor and primary investigator of a randomised clinical trial comparing a higher versus lower oxygenation target in adult patients with hypoxaemic respiratory failure acutely admitted to the intensive care unit (the Handling Oxygenation Targets in COVID‐19 (HOT‐COVID) trial (NCT04425031)).
Marija Barbateskovic: Innovation Fund Denmark provided a grant to Centre for Research in Intensive Care (CRIC), which made it possible for Copenhagen Trial Unit as a partner of CRIC to write the primary review during Marija Barbateskovic’s PhD study.
Figures






























































































Update of
-
Higher versus lower fraction of inspired oxygen or targets of arterial oxygenation for adults admitted to the intensive care unit.Cochrane Database Syst Rev. 2019 Nov 27;2019(11):CD012631. doi: 10.1002/14651858.CD012631.pub2. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2023 Sep 13;9:CD012631. doi: 10.1002/14651858.CD012631.pub3. PMID: 31773728 Free PMC article. Updated.
References
References to studies included in this review
Asfar 2017 {published data only}
-
- Asfar P, Schortgen F, Boisramé-Helms J, Charpentier J, Guérot E, Megarbane B, et al. Hyperoxia and hypertonic saline in patients with septic shock (HYPERS2S): a two-by-two factorial, multicentre, randomised, clinical trial. Lancet Respiratory Medicine 2017;5(3):180-90. [DOI: 10.1016/S2213-2600(17)30046-2] [PMID: ] - DOI - PubMed
Barrot 2020 {published data only}
Gelissen 2021 {published data only}
-
- Gelissen H, Grooth HJ, Smulders Y, Wils E, Ruijter W, Vink R, et al. Effect of low-normal vs high-normal oxygenation targets on organ dysfunction in critically ill patients: a randomized clinical trial. Journal of American Medical Association 2021;326(10):940-8. [DOI: 10.1001/jama.2021.13011] [PMID: ] - DOI - PMC - PubMed
Girardis 2016 {published data only}
-
- Girardis M, Busani S, Damiani E, Donati A, Rinaldi L, Marudi A, et al. Effect of conservative vs conventional oxygen therapy on mortality among patients in an intensive care unit: the oxygen-ICU randomized clinical trial. Journal of American Medical Association 2016;316(15):1583-9. [DOI: 10.1001/jama.2016.11993] [PMID: ] - DOI - PubMed
Gomersall 2002 {published data only}
-
- Gomersall CD, Joynt GM, Freebairn RC, Lai CK, Oh TE. Oxygen therapy for hypercapnic patients with chronic obstructive pulmonary disease and acute respiratory failure: a randomized, controlled pilot study. Critical Care Medicine 2002;30(1):113-6. [DOI: 10.1097/00003246-200201000-00018] [PMID: ] - DOI - PubMed
Ishii 2018 {published data only}
-
- Ishii K, Morimatsu H, Hyodo T, Ono K, Hidaka H, Koyama Y, et al. Relationship between inspired oxygen concentration and atelectasis formation after extubation. Critical Care Medicine 2018;46(1 Suppl 1):533. [DOI: 10.1097/01.ccm.0000529104.66235.9e] - DOI
Jakkula 2018 {published data only}
-
- Jakkula P, Reinikainen M, Hästbacka J, Loisa P, Tiainen M, Pettilä V, et al. Targeting two different levels of both arterial carbon dioxide and arterial oxygen after cardiac arrest and resuscitation: a randomised pilot trial. Intensive Care Medicine 2018;44(12):2112-21. [DOI: 10.1007/s00134-018-5453-9] [PMID: ] - DOI - PMC - PubMed
Jun 2019 {published data only}
-
- Jun J, Sun L, Wang Y, Liu F, Yang G, Han B. Invasive mechanical ventilation with high concentration oxygen therapy for AECOPD patients with acute myocardial infarction. Chest 2019;156(4 Suppl):A958. [DOI: 10.1016/j.chest.2019.08.886] - DOI
Lång 2018 {published data only}
Mackle 2020 {published data only}
-
- Mackle D, Bellomo R, Bailey M, Beasley R, Deane A, Eastwood G, et al, The ICU-ROX Investigators and the Australian and New Zealand Intensive Care Society Clinical Trials Group. Conservative oxygen therapy during mechanical ventilation in the ICU. New England Journal of Medicine 2020;382(11):989-98. [DOI: ] [PMID: ] - PubMed
Martin 2021 {published data only}
-
- Martin DS, McNeil M, Brew-Graves C, Filipe H, O’Driscoll R, Stevens JL, et al. A feasibility randomised controlled trial of targeted oxygen therapy in mechanically ventilated critically ill patients. Journal of the Intensive Care Society 2021;22(4):280-7. [DOI: 10.1177/17511437211010031] - DOI - PMC - PubMed
Mazdeh 2015 {published data only}
-
- Mazdeh M, Taher A, Torabian S, Seifirad S. Effects of normobaric hyperoxia in severe acute stroke: a randomized controlled clinical trial study. Acta Medica Iranica 2015;53(11):676-80. [PMID: ] - PubMed
Panwar 2016 {published data only}
-
- Panwar R, Hardie M, Bellomo R, Barrot L, Eastwood GM, Young PJ, et al. Conservative versus liberal oxygenation targets for mechanically ventilated patients – a pilot multicenter randomized controlled trial. American Journal of Respiratory and Critical Care Medicine 2016;193(1):43-51. [DOI: 10.1164/rccm.201505-1019OC] [PMID: ] - DOI - PubMed
Schjørring 2021 {published data only}
Schmidt 2022 {published data only}
Semler 2022 {published data only}
Taher 2016 {published data only}
Yang 2019 {published data only}
Yang 2021 {published data only}
References to studies excluded from this review
Ahimahalle 2019 {published data only}
-
- Ahimahalle TZ, Amirfarhangi A, Jabbari M, Jenabi A, Bagherzadegan H, Noghabaei G. Impact of oxygen therapy to ameliorate contrast-induced nephropathy in patients with acute coronary syndrome undergoing emergency angiography; a double-blinded clinical trial. Journal of Renal Injury Prevention 2019;8(4):283-8. [DOI: 10.15171/jrip.2019.52] - DOI
Ali 2013 {published data only}
-
- Ali K, Warusevitane A, Lally F, Sim J, Sills S, Pountain S, et al. The stroke oxygen pilot study: a randomized controlled trial of the effects of routine oxygen supplementation early after acute stroke – effect on key outcomes at six months. PLOS One 2013;8(6):e59274. [DOI: 10.1371/journal.pone.0059274] [PMID: ] - DOI - PMC - PubMed
Amar 1994 {published data only}
Austin 2010 {published data only}
Baekgaard 2019 {published data only}
Bardsley 2018 {published data only}
-
- Bardsley G, Pilcher J, McKinstry S, Shirtcliffe P, Berry J, Fingleton J, et al. Oxygen versus air-driven nebulisers for exacerbations of chronic obstructive pulmonary disease: a randomised controlled trial. BMC Pulmonary Medicine 2018;18(1):157. [DOI: 10.1186/s12890-018-0720-7] [PMID: ] - DOI - PMC - PubMed
Bickel 2011 {published data only}
Bray 2018 {published data only}
-
- Bray JE, Hein C, Smith K, Stephenson M, Grantham H, Finn J. Oxygen titration after resuscitation from out-of-hospital cardiac arrest: a multi-centre, randomised controlled pilot study (the EXACT pilot trial). Resuscitation 2018;128:211-5. [DOI: 10.1016/j.resuscitation.2018.04.019] [PMID: ] - DOI - PubMed
Butler 1987 {published data only}
Cheng 2021 {published data only}
Heidari 2017 {published data only}
-
- Heidari F, Rahzani K, Iranpoor D, Rezaee K. The effect of oxygen on the outcomes of non-ST-segment elevation acute coronary syndromes. International Journal of Cardiology: Metabolic and Endocrine 2017;14:67-71. [DOI: 10.1016/j.ijcme.2016.12.002] - DOI
Hofmann 2017 {published data only}
Huynh Ky 2017 {published data only}
-
- Huynh Ky M, Bouchard PA, Morin J, L'Her E, Sarrazin JF, Lellouche F. Closed-loop adjustment of oxygen flowrate with FreeO2 in patients with acute coronary syndrome: comparison of automated titration with FreeO2 (set at two SpO2 target) and of manual titration. A randomized controlled study. American Journal of Respiratory and Critical Care Medicine 2017;195:A3766.
Khoshnood 2017 {published data only}
-
- Khoshnood A, Akbarzadeh M, Roijer A, Meurling C, Carlsson M, Bhiladvala P, et al. Effects of oxygen therapy on wall-motion score index in patients with ST elevation myocardial infarction – the randomized SOCCER trial. Echocardiography 2017;34(8):1130-7. [DOI: 10.1111/echo.13599] [PMID: ] - DOI - PubMed
Khoshnood 2018 {published data only}
-
- Khoshnood A, Carlsson M, Akbarzadeh M, Bhiladvala P, Roijer A, Nordlund D, et al. Effect of oxygen therapy on myocardial salvage in ST elevation myocardial infarction: the randomized SOCCER trial. European Journal of Emergency Medicine 2018;25(2):78-84. [DOI: 10.1097/MEJ.0000000000000431] [PMID: ] - DOI - PubMed
Kuisma 2006 {published data only}
-
- Kuisma M, Boyd J, Voipio V, Alaspää A, Roine RO, Rosenberg P. Comparison of 30 and the 100% inspired oxygen concentrations during early post-resuscitation period: a randomised controlled pilot study. Resuscitation 2006;69(2):199-206. [DOI: 10.1016/j.resuscitation.2005.08.010] [PMID: ] - DOI - PubMed
Meyhoff 2009 {published data only}
-
- Meyhoff CS, Wetterslev J, Jorgensen LN, Henneberg SW, Høgdall C, Lundvall L, et al. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. Journal of American Medical Association 2009;302(14):1543-50. [DOI: 10.1001/jama.2009.1452] [PMID: ] - DOI - PubMed
Mokhtari 2020 {published data only}
-
- Mokhtari A, Akbarzadeh M, Sparv D, Bhiladvala P, Arheden H, Erlinge D, et al. Oxygen therapy in patients with ST elevation myocardial infarction based on the culprit vessel: results from the randomized controlled SOCCER trial. BMC Emergency Medicine 2020;20(1):12. [DOI: 10.1186/s12873-020-00309-y] [PMID: ] - DOI - PMC - PubMed
Padma 2010 {published data only}
Perrin 2011 {published data only}
Ranchord 2012 {published data only}
Rawles 1976 {published data only}
Rodrigo 2003 {published data only}
Roffe 2010 {published data only}
-
- Roffe C, Sills S, Pountain SJ, Allen M. A randomized controlled trial of the effect of fixed-dose routine nocturnal oxygen supplementation on oxygen saturation in patients with acute stroke. Journal of Stroke and Cerebrovascular Diseases 2010;19(1):29-35. [DOI: 10.1016/j.jstrokecerebrovasdis.2009.02.008] [PMID: ] - DOI - PubMed
Roffe 2017 {published data only}
-
- Roffe C, Nevatte T, Sim J, Bishop J, Ives N, Ferdinand P, et al. Effect of routine low-dose oxygen supplementation on death and disability in adults with acute stroke: the stroke oxygen study randomized clinical trial. Journal of American Medical Association 2017;318(12):1125-35. [DOI: 10.1001/jama.2017.11463] [PMID: ] - DOI - PMC - PubMed
Sepehrvand 2019 {published data only}
Sills 2003 {published data only}
-
- Sills S, Halim M, Roffe C. A pilot study of routine nocturnal oxygen supplementation in patients with acute stroke. Age and Ageing 2003;32(Suppl 2):ii41.
Singhal 2005 {published data only}
Singhal 2013 {published data only}
-
- Singhal A, on Behalf of Partners SPOTRIAS Investigators. A phase IIb clinical trial of normobaric oxygen therapy (NBO) in acute ischemic stroke (AIS) (S02.001). Neurology 2013;80(7 Suppl):S02.001.
Stub 2014 {published data only}
Ukholkina 2005 {published data only}
-
- Ukholkina GB, Kostianov IIu, Kuchkina NV, Grendo EP, Gofman IaB. Effect of oxygenotherapy used in combination with reperfusion in patients with acute myocardial infarction. Kardiologiia 2005;45(5):59. [PMID: ] - PubMed
Wu 2014 {published data only}
-
- Wu J, Nevatte T, Roffe C. The stroke oxygen supplementation (S02S) study: comparison of postal and telephone responses of 12 months questionnaire follow up. International Journal of Stroke 2014;9(Suppl 4):37.
Young 2014 {published data only}
-
- Young P, Bailey M, Bellomo R, Bernard S, Dicker B, Freebairn R, et al. HyperOxic Therapy OR NormOxic Therapy after out-of-hospital cardiac arrest (HOT OR NOT): a randomised controlled feasibility trial. Resuscitation 2014;85(12):1686-91. [DOI: 10.1016/j.resuscitation.2014.09.011] [PMID: ] - DOI - PubMed
Young 2017 {published data only}
-
- Young PJ, Mackle DM, Bailey MJ, Beasley RW, Bennett VL, Deane AM, et al. Intensive care unit randomised trial comparing two approaches to oxygen therapy (ICU-ROX): results of the pilot phase. Critical Care and Resuscitation 2017;19(4):344-54. [PMID: ] - PubMed
Zughaft 2013 {published data only}
References to ongoing studies
ACTRN12620000391976 {published data only}
-
- ACTRN12620000391976. The mega randomised registry trial comparing conservative vs. liberal oxygenation targets [A randomised, registry-embedded, single blinded clinical trial comparing conservative oxygen therapy to liberal oxygen therapy in mechanically ventilated adults in the intensive care unit]. anzctr.org.au/Trial/Registration/TrialReview.aspx?id=379432&isReview... (first received 10 March 2020).
ChiCTR‐INR‐17012800 {published data only}
-
- ChiCTR-INR-17012800. The effect of conservative oxygen therapy in the mechanical ventilation patients. chictr.org.cn/showproj.html?proj=21892 (first received 26 September 2017).
ChiCTR‐IOR‐17011717 {published data only}
-
- ChiCTR-IOR-17011717. Comparing the effects of conservative oxygen therapy vs conventional oxygen therapy on outcomes in critically ill patients [The effects of conservative oxygen therapy vs conventional oxygen therapy on outcomes in critically ill patients: a randomised controlled trial]. chictr.org.cn/showproj.html?proj=19990 (first received 21 June 2017).
CTRI/2020/12/029614 {published data only}
-
- CTRI/2020/12/029614. Liberal use of oxygen in early stage of COVID-19 patients [Early liberal oxygen therapy in COVID-19: an open-labeled randomised control trial]. ctri.nic.in/Clinicaltrials/pdf_generate.php?trialid=49680&EncHid=&am... (first received 2 November 2020).
ISRCTN13384956 {published data only}
-
- ISRCTN13384956. Intensive care unit randomised trial comparing two approaches to oxygen therapy (UK-ROX). isrctn.com/ISRCTN13384956 (first received 8 December 2020).
JPRN‐UMIN000046914 {published data only}
-
- JPRN-UMIN000046914. Early restricted oxygen therapy after resuscitation from cardiac arrest trial [Early restricted oxygen therapy after resuscitation from cardiac arrest trial – ER-OXYTRAC trial]. trialsearch.who.int/Trial2.aspx?TrialID=JPRN-UMIN000046914 (first received 14 February 2022).
NCT02999932 {published data only}
-
- NCT02999932. Pulse Oxygen Saturation (SpO2) Directed Oxygen Therapy (POSDOT) [Effect of low vs high peripheral oxygen saturation (SpO 2 ) directed oxygen therapy on mortality among critically ill patients]. clinicaltrials.gov/show/NCT02999932 (first received 14 December 2016).
NCT04144868 {published data only}
-
- NCT04144868. Safety and efficacy of NBO in acute intracerebral hemorrhage. clinicaltrials.gov/show/NCT04144868 (first received 30 December 2019).
NCT04198077 {published data only}
-
- NCT04198077. Conservative versus conventional oxygen administration in critically ill patients [Conservative vs conventional oxygen administration in critically ill patients: effects on ICU mortality. A multicentre randomized open label clinical trial]. clinicaltrials.gov/show/NCT04198077 (first received 10 December 2019).
NCT04425031 {published data only}
-
- NCT04425031. Handling oxygenation targets in COVID-19 (HOT-COVID) [Handling oxygenation targets in COVID-19 patients with acute hypoxaemic respiratory failure in the intensive care unit: a randomised clinical trial of a lower versus a higher oxygenation target]. clinicaltrials.gov/show/NCT04425031 (first received 5 June 2020).
NCT04824703 {published data only}
-
- NCT04824703. Comparative study between liberal and conservative oxygen therapy in mechanically ventilated intensive care patients. clinicaltrials.gov/show/NCT04824703 (first received 26 March 2021).
NCT05404373 {published data only}
-
- NCT05404373. Treatment duration on normobaric hyperoxia in acute ischemic stroke [The efficacy and safety of normobaric hyperoxia on treatment duration for acute ischemic stroke patients with endovascular treatment]. clinicaltrials.gov/show/NCT05404373 (first received 3 June 2022).
NL7185 {published data only}
-
- NL7185. Arterial oxygenation targets in intensive care patients [ICONIC study − conservative versus conventional oxygenation targets in intensive care patients: study protocol for a randomized clinical trial]. onderzoekmetmensen.nl/en/trial/19970 (first received 20 July 2018).
Additional references
AARC 2002
-
- Kallstrom TJ, American Association for Respiratory Care. AARC clinical practice guideline. Oxygen therapy for adults in the acute care facility – 2002 revision & update. Respiratory Care 2002;47(6):717-20. [PMID: ] - PubMed
ACTRN12613000505707
-
- ACTRN12613000505707. Feasibility and safety of conservative versus liberal oxygen targets in the mechanically ventilated patients [A multicenter pilot study to determine whether the conservative oxygenation strategy is as feasible and safe as liberal oxygenation strategy for the ICU patients requiring invasive mechanical ventilation]. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=364185 (first received 5 May 2013).
ACTRN12615000957594
-
- ACTRN12615000957594. Evaluating the effects of two approaches to oxygen therapy in intensive care unit patients requiring life support (mechanical ventilation) [A multicentre, randomised, single-blinded clinical trial comparing the effect of conservative oxygen therapy with standard care on ventilator-free days in mechanically ventilated adults in the intensive care unit]. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=1261... (first received 15 August 2006).
Adhikari 2010
Alba 2016
ARC 2014
-
- Australian Resuscitation Council. Guideline 11.6.1. targeted oxygen therapy in adult advanced life support; 2014. Available at: https://www.resus.org.nz/assets/Uploads/ANZCOR-Guideline-11.6.1-Targeted... (accessed 17 December 2015).
ARDS Definition Task Force 2012
ARDS Network 2000
-
- Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A, Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. New England Journal of Medicine 2000;342(18):1301-8. [DOI: 10.1056/NEJM200005043421801] [PMID: ] - DOI - PubMed
ATS 2005
-
- American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. American Journal of Respiratory and Critical Care Medicine 2005;171(4):388-416. [DOI: 10.1164/rccm.200405-644ST] [PMID: ] - DOI - PubMed
Bailey 2003
Barbateskovic 2021b
Barbateskovic 2021a
-
- Barbateskovic M, Schjørring OL, Krauss SR, Meyhoff CS, Jakobsen JC, Rasmussen BS, et al. Higher vs lower oxygenation strategies in acutely ill adults: a systematic review with meta-analysis and trial sequential analysis. Chest 2021;159(1):154-73. [DOI: 10.1016/j.chest.2020.07.015] [PMID: ] - DOI - PubMed
Bayes factor calculator 2014
-
- Jakobsen JC, Wetterslev J, Winkel P, Lange T, Gluud C. Bayes factor calculation. https://ctu.dk/tools-and-links/bayes-factor-calculation/ (accessed 13 August 2019).
Begg 1994
-
- Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50(4):1088-101. [PMID: ] - PubMed
Bellomo 2011
Benoît 2002
Brenner 2012
Brok 2008
Brok 2009
-
- Brok J, Thorlund K, Wetterslev J, Gluud C. Apparently conclusive meta-analyses may be inconclusive – trial sequential analysis adjustment of random error risk due to repetitive testing of accumulating data in apparently conclusive neonatal meta-analyses. International Journal of Epidemiology 2009;38(1):287-98. [DOI: 10.1093/ije/dyn188] [PMID: ] - DOI - PubMed
Brower 2004
Budinger 2013
Cabello 2016
Chow 2003
Chu 2018
-
- Chu DK, Kim LH, Young PJ, Zamiri N, Almenawer SA, Jaeschke R, et al. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet 2018;391(10131):1693-705. [DOI: 10.1016/S0140-6736(18)30479-3] [PMID: ] - DOI - PubMed
Crapo 1986
Crapo 1999
Crescioli 2022a
-
- Crescioli E, Klitgaard TL, Poulsen LM, Brand BA, Siegemund M, Grøfte T, et al. Long‑term mortality and health‑related quality of life of lower versus higher oxygenation targets in ICU patients with severe hypoxaemia. Intensive Care Medicine 2022;48(6):714-22. [DOI: 10.1007/s00134-022-06695-0] [PMID: ] - DOI - PMC - PubMed
Crescioli 2022b
-
- Crescioli E, Krejberg KU, Klitgaard TL, Nielsen FM, Barbateskovic M, Skrubbeltrang C, et al. Long-term effects of lower versus higher oxygenation levels in adult ICU patients – a systematic review. Acta Anaesthesiologica Scandinavica 2022;66(8):910-22. [DOI: 10.1111/aas.14107] [PMID: ] - DOI - PMC - PubMed
Cumpstey 2020
-
- Cumpstey AF, Oldman AH, Smith AF, Martin D, Grocott MP. Oxygen targets in the intensive care unit during mechanical ventilation for acute respiratory distress syndrome: a rapid review. Cochrane Database of Systematic Reviews 2020, Issue 9. Art. No: CD013708. [DOI: 10.1002/14651858.CD013708] [PMID: ] - DOI - PMC - PubMed
Cumpstey 2022
Dahl 2015
Damiani 2014
de Graaff 2011
de Jonge 2008
Deeks 2010
-
- Deeks JJ, Higgins JPT. Statistical algorithms in Review Manager 5.1. Cochran, 2010. Available from training.cochrane.org/handbook/current/statistical-methods-revman5 2010.
Dellinger 2013
DeMets 1987
DerSimonian 1986
Donahoe 2011
Eastwood 2012
Egger 1997
Esan 2010
Eskesen 2018
Garattini 2016
Gilbert‐Kawai 2014
Gluud 2011
-
- Gluud C, Thorlund K, Engstrøm J, Wetterslev J, Brok J, Imberger G. User manual for Trial Sequential Analysis (TSA). ctu.dk/wp-content/uploads/2021/03/2017-10-10-TSA-Manual-ENG_ER.pdf (accessed February 2016).
GRADEpro GDT [Computer program]
-
- GRADEpro GDT. Version accessed 25 March 2019. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015. Available at gradepro.org.
Guyatt 2008
-
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al, GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. British Medical Journal 2008;336(7650):924-6. [DOI: 10.1136/bmj.39489.470347.AD] [PMID: ] - DOI - PMC - PubMed
Hafner 2015
Hansen 2021
Harbord 2006
Helmerhorst 2015
-
- Helmerhorst HJ, Roos-Blom MJ, Westerloo DJ, Jonge E. Association between arterial hyperoxia and outcome in subsets of critical illness: a systematic review, meta-analysis, and meta-regression of cohort studies. Critical Care Medicine 2015;43(7):1508-19. [DOI: 10.1097/CCM.0000000000000998] [PMID: ] - DOI - PubMed
Helmerhorst 2017a
Helmerhorst 2017b
-
- Helmerhorst HJF, Schouten LRA, Wagenaar GTM, Juffermans NP, Roelofs JJTH, Schultz MJ, et al. Hyperoxia provokes a time- and dose-dependent inflammatory response in mechanically ventilated mice, irrespective of tidal volumes. Intensive Care Medicine Experimental 2017;5(1):27. [DOI: 10.1186/s40635-017-0142-5] [PMID: ] - DOI - PMC - PubMed
Higgins 2002
Higgins 2003
Higgins 2011a
Higgins 2011b
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from training.cochrane.org/handbook/archive/v5.1/.
Higgins 2016
-
- Higgins JPT, Sterne JAC, Savović J, Page MJ, Hróbjartsson A, Boutron I, et al. A revised tool for assessing risk of bias in randomized trials. In: Chandler J, McKenzie J, Boutron I, Welch V (editors). Cochrane Methods. Cochrane Database of Systematic Reviews, 2016. Available from cochranelibrary.com/cdsr/doi/10.1002/14651858.CD201601/full. [DOI: ]
Higgins 2019
-
- Higgins JPT, Savović J, Page MJ, Sterne JAC. RoB 2: a revised Cochrane risk-of-bias tool for randomized trials. https://sites.google.com/site/riskofbiastool/welcome/rob-2-0-tool/curren... (accessed 22 August 2019).
Higgins 2021
-
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from www.training.cochrane.org/handbook.
Hróbjartsson 2014
-
- Hróbjartsson A, Emanuelsson F, Skou Thomsen AS, Hilden J, Brorson S. Bias due to lack of patient blinding in clinical trials. A systematic review of trials randomizing patients to blind and nonblind sub-studies. International Journal of Epidemiology 2014;43(4):1272-83. [DOI: 10.1093/ije/dyu115] [PMID: ] - DOI - PMC - PubMed
ICH‐GCP 1997
-
- International Council on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use. International conference on harmonisation of technical requirements for registration of pharmaceuticals for human use (ICH) adopts consolidated guideline on good clinical practice in the conduct of clinical trials on medicinal products for human use. International Digest of Health Legislation 1997;48(2):231-4. [PMID: ] - PubMed
Imberger 2015
-
- Imberger G, Gluud C, Boylan J, Wetterslev J. Systematic reviews of anesthesiologic interventions reported as statistically significant: problems with power, precision, and type 1 error protection. Anesthesia and Analgesia 2015;121(6):1611-22. [DOI: 10.1213/ANE.0000000000000892] [PMID: ] - DOI - PubMed
Imberger 2016
IRCT201212199647N2
-
- IRCT201212199647N2. Effect of high percent oxygen therapy in compared without oxygen therapy on rehabilitation in the first 12 hours of admission in patients with stroke: a randomized clinical trial. en.irct.ir/trial/10208 (first received 3 November 2013).
Itagaki 2015
Jakobsen 2014a
Jakobsen 2014b
-
- Jakobsen JC, Gluud C, Winkel P, Lange T, Wetterslev J. The thresholds for statistical and clinical significance – a five-step procedure for evaluation of intervention effects in randomised clinical trials. BMC Medical Research Methodology 2014;14:34. [DOI: 10.1186/1471-2288-14-34] [PMID: ] - DOI - PMC - PubMed
Jakobsen 2016
-
- Jakobsen JC, Wetterslev J, Lange T, Gluud C. Comment on: Taking into account risks of random errors when analysing multiple outcomes in systematic reviews. www.cochranelibrary.com/cdsr/doi/10.1002/14651858.ED000111/full 18 March 2016. [DOI: 10.1002/14651858.ED000111] [PMID: ] - DOI - PMC - PubMed
Kahn 2010
Kallet 2013
Kenmure 1971
Kent 2011
Kilgannon 2010
-
- Kilgannon JH, Jones AE, Shapiro NI, Angelos MG, Milcarek B, Hunter K, et al, Emergency Medicine Shock Research Network (EMShockNet) Investigators. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. Journal of the American Medical Association 2010;303(21):2165-71. [DOI: 10.1001/jama.2010.707] [PMID: ] - DOI - PubMed
Kraft 2018
Kratz 2004
Kulinskaya 2014
Lefebvre 2021
-
- Lefebvre C, Glanville J, Briscoe S, Littlewood A, Marshall C, Metzendorf M-I, et al. Chapter 4: Searching for and selecting studies. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available from training.cochrane.org/handbook.
Li 2021a
Li 2021b
-
- Li X, Liu D, Liu C, Mao Z, Liu Y, Yi H, et al. Conservative versus liberal oxygen therapy in relation to all-cause mortality among patients in the intensive care unit: a systematic review of randomized controlled trials with meta-analysis and trial sequential analysis. Medicina Intensiva 2023;47(2):73-83. [DOI: 10.1016/j.medin.2021.08.006] [PMID: ] - DOI - PubMed
MAGIC 2002
-
- Magnesium in Coronaries (MAGIC) Trial Investigators. Early administration of intravenous magnesium to high-risk patients with acute myocardial infarction in the Magnesium in Coronaries (MAGIC) Trial: a randomised controlled trial. Lancet 2002;360(9341):1189-96. [DOI: 10.1016/s0140-6736(02)11278-5] [PMID: ] - DOI - PubMed
Mantel 1959
-
- Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. Journal of the National Cancer Institute 1959;22(4):719-48. [PMID: ] - PubMed
Mascha 2015
Metnitz 2009
Meyhoff 2012
-
- Meyhoff CS, Jorgensen LN, Wetterslev J, Christensen KB, Rasmussen LS, PROXI Trial Group. Increased long-term mortality after a high perioperative inspiratory oxygen fraction during abdominal surgery: follow-up of a randomized clinical trial. Anesthesia and Analgesia 2012;115(4):849-54. [DOI: 10.1213/ANE.0b013e3182652a51] [PMID: ] - DOI - PubMed
NCT01201291
-
- NCT01201291. Impact of inspired oxygen fraction on outcome in patients with traumatic brain injury (BRAINOXY). clinicaltrials.gov/ct2/show/NCT01201291 (first received 14 September 2010).
NCT01319643
-
- NCT01319643. Normal oxygenation versus hyperoxia in the intensive care unit (ICU) (OXYGEN-ICU) [Normal oxygenation maintenance in intensive care unit: randomized controlled trial]. clinicaltrials.gov/ct2/show/NCT01319643 (first received 22 March 2011).
NCT01722422
-
- NCT01722422. Hyperoxia and hypertonic saline in septic shock (Hyper2S). clinicaltrials.gov/ct2/show/study/NCT01722422 (first received 6 November 2012).
NCT02321072
-
- NCT02321072. Optimal oxygenation in the intensive care unit (O2-ICU) [The effects of hyperoxia on organ dysfunction and outcome in critically ill patients with SIRS]. clinicaltrials.gov/ct2/show/NCT02321072 (first received 9 December 2014).
NCT02698917
-
- NCT02698917. Carbon dioxide, oxygen and mean arterial pressure after cardiac arrest and resuscitation (COMACARE) [Carbon dioxide, oxygen and mean arterial pressure after cardiac arrest and resuscitation – targeting high vs. low normal values]. clinicaltrials.gov/ct2/show/NCT02698917 (first received 4 March 2016).
NCT02713451
-
- NCT02713451. Liberal oxygenation versus conservative oxygenation in ARDS (LOCO2) [Liberal oxygenation versus conservative oxygenation in patients with acute respiratory distress syndrome: impact on mortality (LOCO 2 study)]. clinicaltrials.gov/ct2/show/NCT02713451 (first received 25 February 2016).
NCT02999932
-
- NCT02999932. Pulse oxygen saturation (SpO2) directed oxygen therapy (POSDOT) [Effect of low vs high peripheral oxygen saturation (SpO 2 ) directed oxygen therapy on mortality among critically ill patients]. clinicaltrials.gov/ct2/show/NCT02999932 (first received 14 December 2016).
NCT03174002
-
- NCT03174002. Handling oxygenation targets in the intensive care unit (HOT-ICU) [Handling oxygenation targets in adults with acute hypoxaemic respiratory failure in the intensive care unit: a randomised clinical trial of a lower versus a higher oxygenation target]. clinicaltrials.gov/ct2/show/NCT03174002 (first received 30 May 2017).
NCT03287466
-
- NCT03287466. Targeted oxygen therapy in critical illness (TOXYC) [A randomised controlled trial of targeted oxygen therapy in mechanically ventilated critically ill patients]. clinicaltrials.gov/ct2/show/NCT03287466 (first received 20 July 2017).
O’Driscoll 2017
-
- O’Driscoll BR, Howard LS, Earis J, Mak V, British Thoracic Society Emergency Oxygen Guideline Group, BTS Emergency Oxygen Guideline Development Group. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax 2017;72(Suppl 1):ii1-90. [DOI: 10.1136/thoraxjnl-2016-209729] [PMID: ] - DOI - PubMed
Palmer 2019
-
- Palmer E, Post B, lapaukh R, Marra G, MacCallum NS, Brealey D, et al. The association between supraphysiologic arterial oxygen levels and mortality in critically ill patients. A multicenter observational cohort study. American Journal of Respiratory and Critical Care Medicine 2019;200(11):1373-80. [DOI: 10.1164/rccm.201904-0849OC] [PMID: ] - DOI - PMC - PubMed
Pannu 2016
Panwar 2013
Patrona 2014
-
- Patrona SD, Zanini A, Aiello M, Adamo D, Casale S, Cherubino F, et al. Estimation of minimum clinically important difference in EQ-VAS score after pulmonary rehabilitation in COPD patients. European Respiratory Journal 2014;44(Suppl 58):P3669.
Petersson 2014
Pickard 2007
Pocock 2015
Pogue 1997
Rachmale 2012
Raj 2013
Raoof 2010
Review Manager 2020 [Computer program]
-
- Review Manager 5 (RevMan 5). Version 5.4. Copenhagen: The Cochrane Collaboration, 2020.
Rodríguez‐Roisin 2005
Rothen 1995a
Rothen 1995b
Roussos 2003
Sacco 2013
-
- Sacco RL, Kasner SE, Broderick JP, Caplan LR, Connors JJ, Culebras A, et al, American Heart Association Stroke Council, Council on Cardiovascular Surgery and Anesthesia, Council on Cardiovascular Radiology and Intervention, Council on Cardiovascular and Stroke Nursing, Council on Epidemiology and Prevention, Council on Peripheral Vascular Disease, Council on Nutrition, Physical Activity and Metabolism. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44(7):2064-89. [DOI: 10.1161/STR.0b013e318296aeca] [PMID: ] - DOI - PMC - PubMed
Savović 2018
-
- Savović J, Turner RM, Mawdsley D, Jones HE, Beynon R, Higgins JPT, et al. Association between risk-of-bias assessments and results of randomized trials in Cochrane Reviews: the ROBES meta-epidemiologic study. American Journal of Epidemiology 2018;187(5):1113-22. [DOI: 10.1093/aje/kwx344] [PMID: ] - DOI - PMC - PubMed
Schjørring 2020
-
- Schjørring OL, Jensen AKG, Nielsen CG, Ciubotariu A, Perner A, Wetterslev J, et al. Arterial oxygen tensions in mechanically ventilated ICU patients and mortality: a retrospective, multicentre, observational cohort study. British Journal of Anaesthesia 2020;124(4):420-29. [DOI: 10.1016/j.bja.2019.12.039] [PMID: ] - DOI - PubMed
Sepehrvand 2018
Siemieniuk 2018
Sinclair 2004
Sjöberg 2013
STATA 2017 [Computer program]
-
- Stata. Version 15. College Station, TX, USA: StataCorp, 2017. Available at www.stata.com.
Sterne 2001
Sterne 2019
Stub 2015
Suzuki 2013
Tan 2014
-
- Tan HL, Wijeweera O. Oxygen in critical care. Trends in Anaesthesia and Critical Care 2014;4(4):102-8. [DOI: 10.1016/j.tacc.2014.05.001] - DOI
Terkawi 2016
-
- Terkawi AS, Mavridis D, Flood P, Wetterslev J, Terkawi RS, Bin Abdulhak AA, et al. Does ondansetron modify sympathectomy due to subarachnoid anesthesia?: meta-analysis, meta-regression, and trial sequential analysis. Anesthesiology 2016;124(4):846-69. [DOI: 10.1097/ALN.0000000000001039] [PMID: ] - DOI - PubMed
Thorlund 2009
Thygesen 2012
-
- Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, Joint ESC/ACCF/AHA/WHF Task Force for Universal Definition of Myocardial Infarction, Authors/Task Force Members Chairpersons, Biomarker Subcommittee, ECG Subcommittee, Imaging Subcommittee, Classification Subcommittee, et al. Third universal definition of myocardial infarction. Journal of American College of Cardiology 2012;60(16):1581-98. [DOI: 10.1016/j.jacc.2012.08.001] [PMID: ] - DOI - PubMed
TSA 2011 [Computer program]
-
- Trial sequential analysis. Version 0.9 Beta. Copenhagen: Copenhagen Trial Unit, 2011. www.ctu.dk/tsa/downloads.aspx.
Turner 2013
van der Wal 2022
-
- Wal LI, Grim CCA, Westerloo DJ, Schultz MJ, Jonge E, Helmerhorst HJF. Higher versus lower oxygenation strategies in the general intensive care unit population: a systematic review, meta-analysis and meta-regression of randomized controlled trials. Journal of Critical Care 2022;72:154151. [DOI: 10.1016/j.jcrc.2022.154151] [PMID: ] - DOI - PubMed
Wagner 1977
Watson 2000
-
- Watson NA, Beards SC, Altaf N, Kassner A, Jackson A. The effect of hyperoxia on cerebral blood flow: a study in healthy volunteers using magnetic resonance phase-contrast angiography. European Journal of Anaesthesiology 2000;17(3):152-9. [DOI: 10.1046/j.1365-2346.2000.00640.x] [PMID: ] - DOI - PubMed
Wetterslev 2008
Wetterslev 2009
Wetterslev 2015
Whitehead 2002
Woods 2002
Wunsch 2010
You 2018
Young 2012
-
- Young P, Beasley R, Bailey M, Bellomo R, Eastwood GM, Nichol A, et al, Study of Oxygen in Critical Care (SOCC) Group. The association between early arterial oxygenation and mortality in ventilated patients with acute ischaemic stroke. Critical Care and Resuscitation 2012;14(1):14-9. [PMID: ] - PubMed
Young 2017
-
- Young PJ, Mackle DM, Bailey MJ, Beasley RW, Bennett VL, Deane AM, et al, The ICU-ROX pilot investigators, The Australian and New Zealand Intensive Care Society Clinical Trials Group. Intensive care unit randomised trial comparing two approaches to oxygen therapy (ICU-ROX): results of the pilot phase. Critical Care and Resuscitation 2017;19(4):344-54. [PMID: ] - PubMed
Young 2021
-
- Young PJ, Bailey M, Bellomo R, Bernard S, Bray J, Jakkula P, et al. Conservative or liberal oxygen therapy in adults after cardiac arrest: an individual-level patient data meta-analysis of randomised controlled trials. Resuscitation 2020;157:15-22. [DOI: 10.1016/j.resuscitation.2020.09.036.] [PMID: ] - DOI - PubMed
Zaher 2007
Zanini 2015
-
- Zanini A, Aiello M, Adamo D, Casale S, Cherubino F, Patrona SD, et al. Estimation of minimal clinically important difference in EQ-5D visual analog scale score after pulmonary rehabilitation in subjects with COPD. Respiratory Care 2015;60(1):88-95. [DOI: 10.4187/respcare.03272] [PMID: ] - DOI - PubMed
References to other published versions of this review
Barbateskovic 2017
-
- Barbateskovic M, Schjørring OL, Jakobsen JC, Meyhoff CS, Dahl RM, Rasmussen BS, et al. Higher versus lower inspiratory oxygen fraction or targets of arterial oxygenation for adult intensive care patients. Cochrane Database of Systematic Reviews 2017, Issue 4. Art. No: CD012631. [DOI: 10.1002/14651858.CD012631] - DOI
Barbateskovic 2019
-
- Barbateskovic M, Schjørring OL, Krauss SR, Jakobsen JC, Meyhoff CS, Dahl RM, et al. Higher versus lower fraction of inspired oxygen or targets of arterial oxygenation for adults admitted to the intensive care unit. Cochrane Database of Systematic Reviews 2019, Issue 11. Art. No: CD012631. [DOI: 10.1002/14651858.CD012631.pub2] [PMID: ] - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical