

Efficacy and safety of combined Chinese and Western medicine in the treatment of knee osteoarthritis: a prospective, multicenter cohort study
- PMID: 37701040
- PMCID: PMC10494435
- DOI: 10.3389/fphar.2023.1176980
Efficacy and safety of combined Chinese and Western medicine in the treatment of knee osteoarthritis: a prospective, multicenter cohort study
Abstract
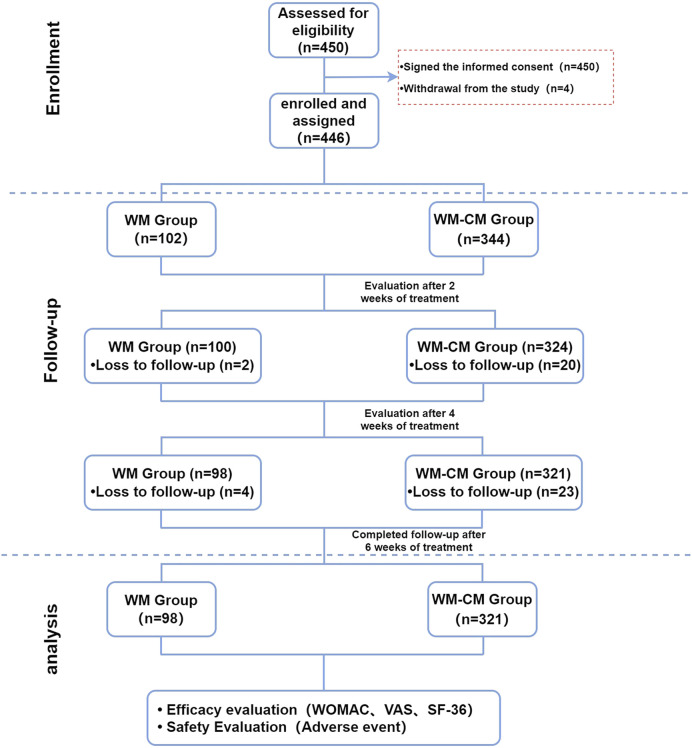
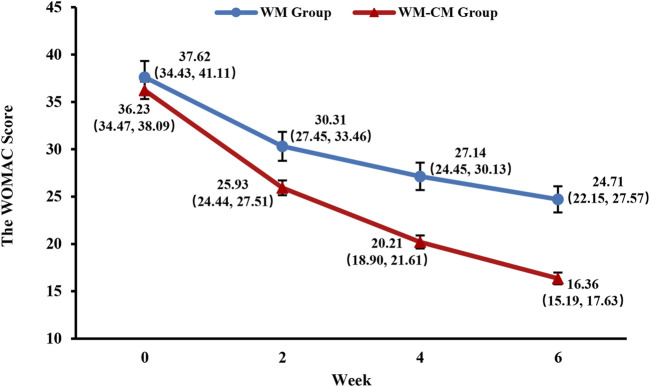
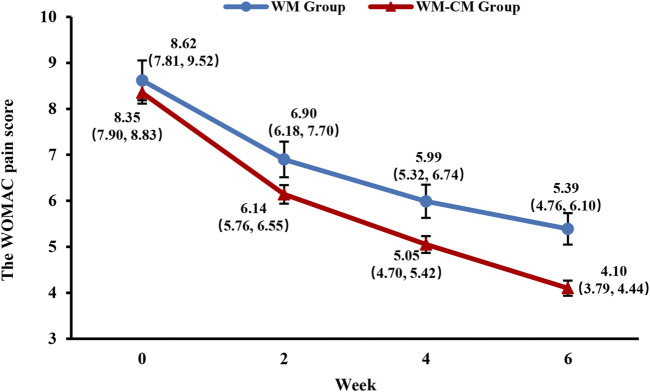
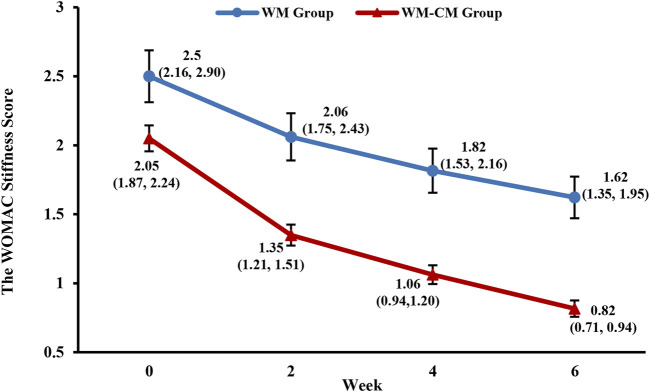
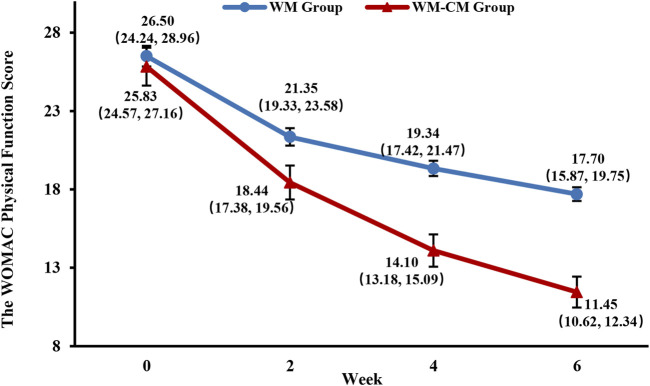
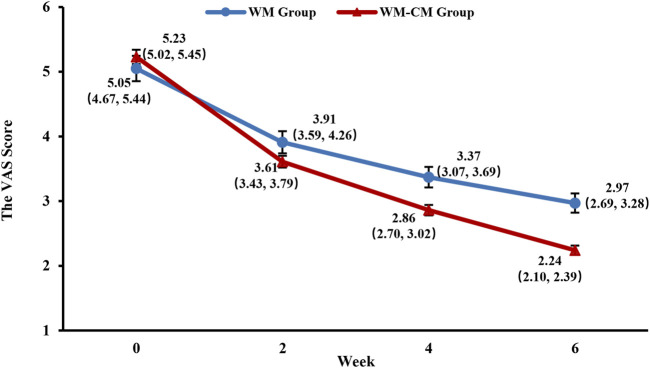
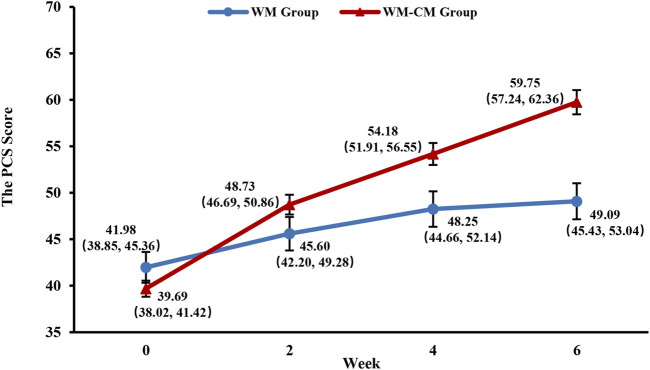
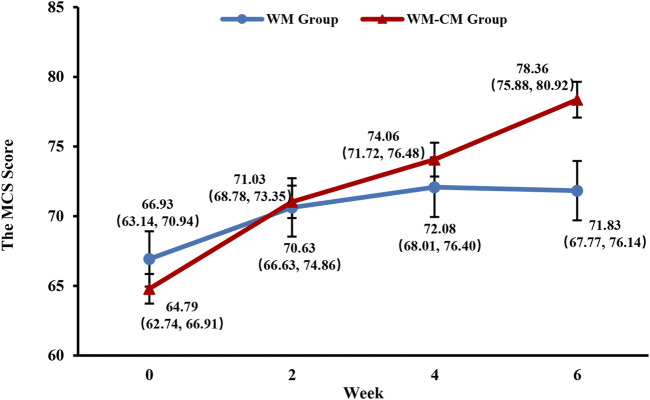
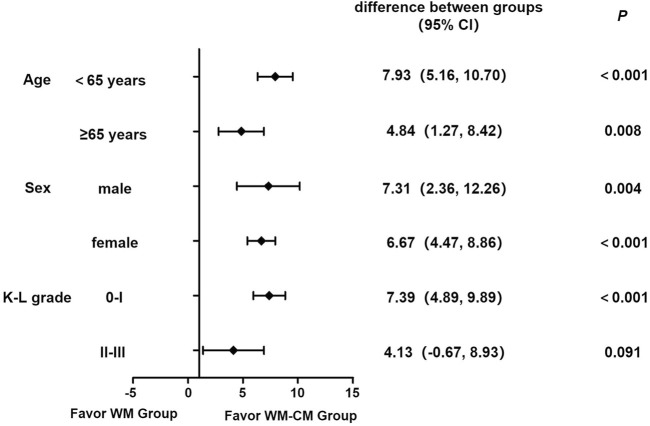
Purpose: To conduct a real-world evaluation of the efficacy and safety of combined Chinese and Western medicine in treating knee osteoarthritis (KOA). Methods: A multicenter, prospective cohort study design was employed, enrolling 450 KOA patients (Kellgren-Lawrence score of 3 or less). The patients were divided into a Western medicine treatment group (WM group) and a combined Western and traditional Chinese medicine treatment group (WM-CM group). A 6-week treatment plan was administered, and follow-up visits occurred at 2 weeks, 4 weeks, and 6 weeks after initiating treatment. The primary outcome indicator was the total Western Ontario and McMaster Universities Arthritis Index (WOMAC) score after 6 weeks of treatment. Secondary outcome indicators included WOMAC subscales for pain, stiffness, and joint function, visual analogue scale (VAS) score, physical component summary (PCS), mental component summary (MCS), and clinical effectiveness. The incidence of drug-related adverse events was used as a safety evaluation indicator. Results: A total of 419 patients were included in the final analysis: 98 in the WM group and 321 in the WM-CM group. The baseline characteristics of the two groups were comparable, except for the incidence of stiffness symptoms and stiffness scores. After 6 weeks of treatment, the WM-CM group exhibited superior results to the WM group in improving the total WOMAC score (24.71 ± 1.38 vs. 16.36 ± 0.62, p < 0.001). The WM-CM group also outperformed the WM group in WOMAC pain and joint function scores, VAS score, PCS score, MCS score, and clinical effectiveness (p < 0.05), which was consistent with the findings of the main evaluation index. Subgroup analysis indicated that the combined Chinese and Western medicine treatment showed more pronounced benefits in patients under 65 years of age and in those with a Kellgren-Lawrence (K-L) classification of 0-I. Throughout the study, no adverse effects were observed in either group. Conclusion: The combination of Chinese and Western medicine demonstrated superiority over Western medicine alone in relieving knee pain symptoms, improving knee function, and enhancing the quality of life for KOA patients with a K-L score of 3 or less. Moreover, the treatment exhibited a good safety profile. Clinical Trial Registration: (https://www.chictr.org.cn/), identifier (ChiCTR1900027175).
Keywords: combined Chinese and Western medicine; efficacy; knee osteoarthritis; prospective cohort; real-world study.
Copyright © 2023 Ye, Lin, Hu, Yang, Zheng, Li, Zhong, Wang, Zhang, Luo, Xiao, Wu, Li, Zou, Li, Li, Wang, Yang, Zhu, Han and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical efficacy of Osteoking in knee osteoarthritis therapy: a prospective, multicenter, non-randomized controlled study in China.Front Pharmacol. 2024 Jun 28;15:1381936. doi: 10.3389/fphar.2024.1381936. eCollection 2024. Front Pharmacol. 2024. PMID: 39005940 Free PMC article.
-
Efficacy and safety of Tuina (Chinese Therapeutic Massage) for knee osteoarthritis: A randomized, controlled, and crossover design clinical trial.Front Med (Lausanne). 2023 Apr 5;10:997116. doi: 10.3389/fmed.2023.997116. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37089612 Free PMC article.
-
[Point-pricking method with fire needle for knee osteoarthritis: a randomized controlled trial].Zhen Ci Yan Jiu. 2022 Oct 25;47(10):902-6. doi: 10.13702/j.1000-0607.20210745. Zhen Ci Yan Jiu. 2022. PMID: 36301168 Clinical Trial. Chinese.
-
The Effectiveness and Safety of Moxibustion for Treating Knee Osteoarthritis: A PRISMA Compliant Systematic Review and Meta-Analysis of Randomized Controlled Trials.Pain Res Manag. 2019 Dec 17;2019:2653792. doi: 10.1155/2019/2653792. eCollection 2019. Pain Res Manag. 2019. PMID: 31949547 Free PMC article.
-
The Efficacy and Safety of Chinese Herbal Medicine in the Treatment of Knee Osteoarthritis: An Updated Systematic Review and Meta-Analysis of 56 Randomized Controlled Trials.Oxid Med Cell Longev. 2022 Jan 7;2022:6887988. doi: 10.1155/2022/6887988. eCollection 2022. Oxid Med Cell Longev. 2022. PMID: 35035664 Free PMC article.
Cited by
-
Effects of platelet-rich plasma combined with isometric quadriceps contraction on cartilage in a rat model of knee osteoarthritis.Regen Ther. 2024 Jul 15;26:469-477. doi: 10.1016/j.reth.2024.06.021. eCollection 2024 Jun. Regen Ther. 2024. PMID: 39070125 Free PMC article.
-
Clinical efficacy of Osteoking in knee osteoarthritis therapy: a prospective, multicenter, non-randomized controlled study in China.Front Pharmacol. 2024 Jun 28;15:1381936. doi: 10.3389/fphar.2024.1381936. eCollection 2024. Front Pharmacol. 2024. PMID: 39005940 Free PMC article.
-
A Review of Advances in Multimodal Treatment Strategies for Chronic Disorders of Consciousness Following Severe Traumatic Brain Injury.Int J Gen Med. 2025 Feb 14;18:771-786. doi: 10.2147/IJGM.S502086. eCollection 2025. Int J Gen Med. 2025. PMID: 39967766 Free PMC article. Review.
-
Chinese herbal medicine for chronic pain: a bibliometric analysis based on integrated databases (2011-2024).Front Med (Lausanne). 2025 Aug 8;12:1642093. doi: 10.3389/fmed.2025.1642093. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40861240 Free PMC article.
-
Natural Compounds for Preventing Age-Related Diseases and Cancers.Int J Mol Sci. 2024 Jul 9;25(14):7530. doi: 10.3390/ijms25147530. Int J Mol Sci. 2024. PMID: 39062777 Free PMC article. Review.
References
-
- Angst F., Aeschlimann A., Stucki G. (2001). Smallest detectable and minimal clinically important differences of rehabilitation intervention with their implications for required sample sizes using WOMAC and SF-36 quality of life measurement instruments in patients with osteoarthritis of the lower extremities. Arthritis Rheum. 45 (4), 384–391. 10.1002/1529-0131(200108)45:4<384:AID-ART352>3.0.CO;2-0 - DOI - PubMed
-
- Belk J. W., Kraeutler M. J., Houck D. A., Goodrich J. A., Dragoo J. L., McCarty E. C. (2021). Platelet-rich plasma versus hyaluronic acid for knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. Am. J. Sports Med. 49 (1), 249–260. 10.1177/0363546520909397 - DOI - PubMed
-
- Blumenthal K. G., Lai K. H., Huang M., Wallace Z. S., Wickner P. G., Zhou L. (2017). Adverse and hypersensitivity reactions to prescription nonsteroidal anti-inflammatory agents in a large health care system. J. Allergy Clin. Immunol. Pract. 5 (3), 737–743. 10.1016/j.jaip.2016.12.006 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources