

Multidisciplinary Approach to Sedation and Early Mobility of Intubated Critically Ill Neurologic Patients Improves Mobility at Discharge
- PMID: 37701262
- PMCID: PMC10494812
- DOI: 10.1177/19418744231182897
Multidisciplinary Approach to Sedation and Early Mobility of Intubated Critically Ill Neurologic Patients Improves Mobility at Discharge
Abstract
Background and purpose: Over-sedation may confound neurologic assessment in critically ill neurologic patients and prolong duration of mechanical ventilation (MV). Decreased sedative use may facilitate early functional independence when combined with early mobility. The objective of this study was to evaluate the impact of a stepwise, multidisciplinary analgesia-first sedation pathway and early mobility protocol on medication use and mobility in the neuroscience intensive care unit (ICU).
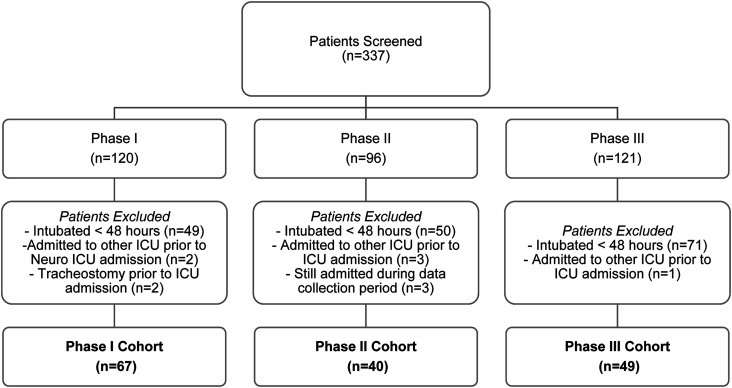
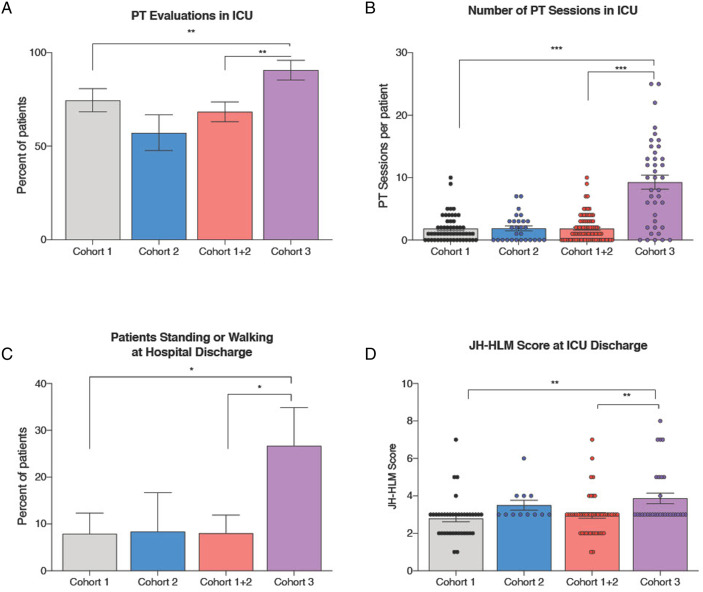
Methods: We performed a single-center prospective cohort study with adult patients admitted to a neuroscience ICU between March and June 2016-2018 who required MV for greater than 48 hours. Patients were included from three separate phases of the study: Phase I - historical controls (2016); Phase II - analgesia-first pathway (2017); Phase III - early mobility protocol (2018). Primary outcomes included propofol requirements during MV, total rehabilitation therapy provided, and functional mobility during ICU admission.
Results: 156 patients were included in the analysis. Decreasing propofol exposure was observed during Phase I, II, and III (median 2243.7 mg/day vs 2065.6 mg/day vs 1360.8 mg/day, respectively; P = .04 between Phase I and III). Early mobility was provided in 59.7%, 40%, and 81.6% of patients while admitted to the ICU in Phase I, II, and III, respectively (P < .01). An increased proportion of patients in Phase III were walking or ambulating at ICU discharge (26.7%; 8/30) compared to Phase I (7.9%, 3/38, P = .05).
Conclusions: An interdisciplinary approach with an analgesia-first sedation pathway with early mobility protocol was associated with less sedative use, increased rehabilitation therapy, and improved functional mobility status at ICU discharge.
Keywords: analgesia; analgosedation; early mobility; neurocritical care; sedation.
© The Author(s) 2023.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.V. and M.B. have no conflicts relevant to this article, this work was conceived and completed during employment at Brigham and Women’s Hospital (H.V. and M.B.) and Massachusetts General Hospital (M.B.), since then, H.V. and M.B. have been employed by Marinus Pharmaceutical Inc. All other authors (C.I., J.T., J.J., L.M., K.L., A.M., P.K., A.B.,) have no conflicts of interest to disclose.
Figures
Similar articles
-
Analgosedation: a paradigm shift in intensive care unit sedation practice.Ann Pharmacother. 2012 Apr;46(4):530-40. doi: 10.1345/aph.1Q525. Epub 2012 Apr 10. Ann Pharmacother. 2012. PMID: 22496477 Review.
-
[Effect of early off-bed mobility on delirium in mechanical ventilated patients in intensive care unit: a prospective randomized controlled study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Nov;33(11):1353-1357. doi: 10.3760/cma.j.cn121430-20210209-00238. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 34980307 Clinical Trial. Chinese.
-
Clinical sedation scores as indicators of sedative and analgesic drug exposure in intensive care unit patients.Am J Geriatr Pharmacother. 2007 Sep;5(3):218-31. doi: 10.1016/j.amjopharm.2007.10.005. Am J Geriatr Pharmacother. 2007. PMID: 17996661
-
An analgesia-delirium-sedation protocol for critically ill trauma patients reduces ventilator days and hospital length of stay.J Trauma. 2008 Sep;65(3):517-26. doi: 10.1097/TA.0b013e318181b8f6. J Trauma. 2008. PMID: 18784563
-
Optimal intravenous dosing strategies for sedatives and analgesics in the intensive care unit.Crit Care Clin. 1995 Oct;11(4):827-47. Crit Care Clin. 1995. PMID: 8535981 Review.
References
-
- Lele A, Souter MJ. Sedation practices in the Neurocritical Care Unit. J Neuroanaesth Crit Care. 2016;03:81-87.
LinkOut - more resources
Full Text Sources