

Trends in Distal Radius Fixation Reimbursement, Charge, and Utilization in the Medicare Population
- PMID: 37701309
- PMCID: PMC10495210
- DOI: 10.1055/s-0042-1748781
Trends in Distal Radius Fixation Reimbursement, Charge, and Utilization in the Medicare Population
Abstract
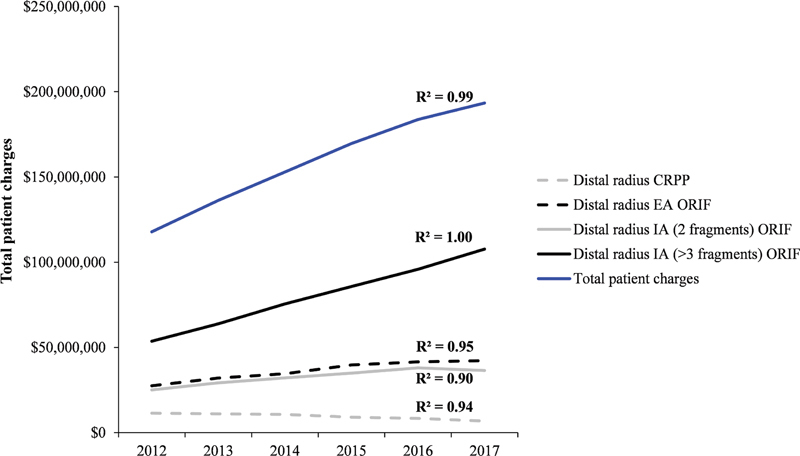
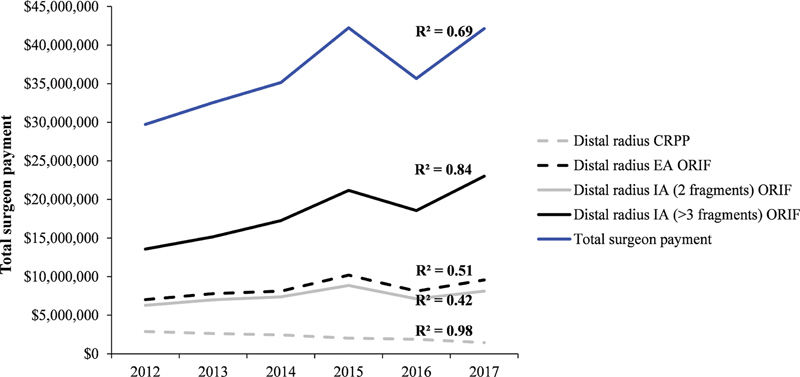
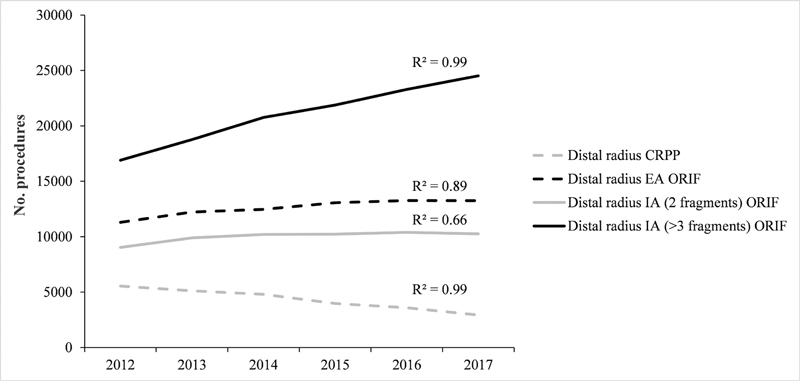
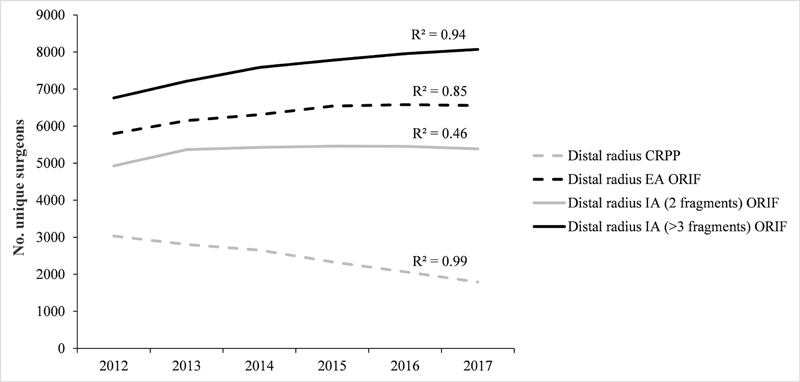
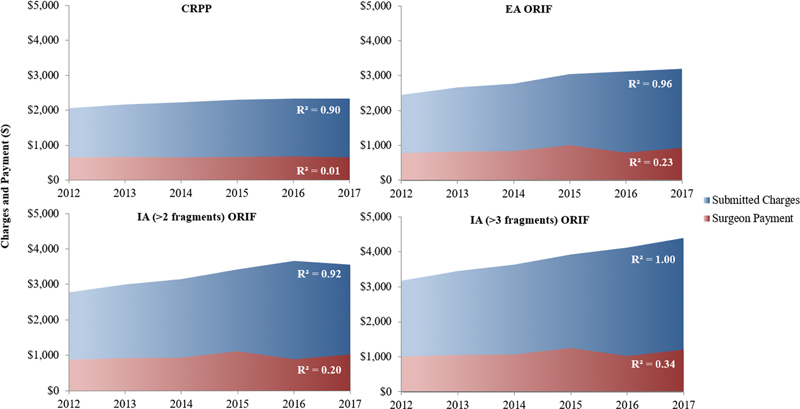
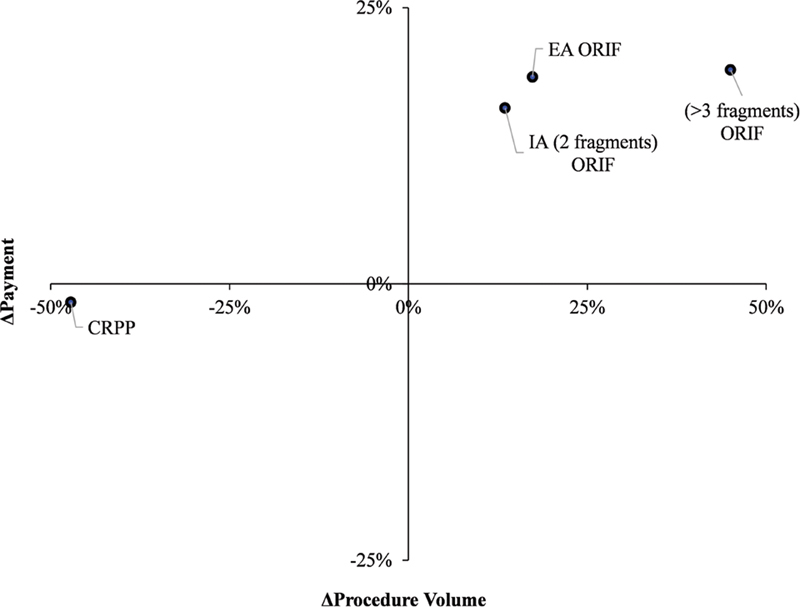
Background Distal radius fractures (DRF) are the second most common fragility fracture experienced by the elderly, and surgical management constitutes an appreciable sum of Medicare expenditure for upper extremity surgery. Using Medicare data from 2012 to 2017, our primary aim was to describe temporal changes in surgical treatment, physician payment, and patient charges for DRF fixation. Methods We examined surgical volumes and retrospective patient charge (services billed by surgeon) and surgeon payment (professional fee) data from 2012 to 2017 for four DRF surgeries: closed reduction percutaneous pinning (CRPP), open reduction internal fixation (ORIF) of extra-articular fractures, ORIF of intra-articular (IA) (2-fragment) fractures, and ORIF of IA (> 3 fragments) fractures. The reimbursement ratio was defined and calculated as the ratio of charges to payment. Rates were adjusted for inflation using the annual consumer-price index. Results For these four surgeries from 2012 to 2017, total patient charges grew by 64% from $117 to 193 million, while surgeon payment grew by 42% from $30 to 42 million. CRPP cases fell by 47%, while ORIF increased by 17, 14, and 45% for extra-articular, IA (2-fragment), and IA (> 3 fragments) surgeries, respectively. After adjusting for inflation, payment to physicians increased by more than or equal to 16% for all procedures except for CRPP, which fell by 2%. Charges during this same period increased from 13 to 38%. Reimbursement ratios declined from -9.2% to -13% for each procedure. Conclusion From 2012 to 2017, while charges have outpaced surgeon payment, payment has outpaced inflation for all forms of distal radius ORIF, aside from CRPP. There has been a continued sharp decline of CRPP. Level of Evidence is III, economic.
Keywords: closed reduction percutaneous fixation; distal radius fracture; patient charges; surgeon payment; volar plates.
Society of Indian Hand Surgery & Microsurgeons. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
Are We Working Harder for Less Pay? A Survey of Medicare Reimbursement for Hand and Upper Extremity Surgery.Plast Reconstr Surg. 2022 Apr 1;149(4):711e-719e. doi: 10.1097/PRS.0000000000008906. Plast Reconstr Surg. 2022. PMID: 35157616
-
Increased Reimbursement for Surgical Fixation of Hip Fractures: The Difference Between the Hospital and the Surgeon.J Orthop Trauma. 2021 Jul 1;35(7):339-344. doi: 10.1097/BOT.0000000000002092. J Orthop Trauma. 2021. PMID: 34131086
-
Does open reduction internal fixation using a volar locking plate and closed reduction percutaneous pinning using K wires provide similar functional and radiological outcomes for unstable distal radius fractures?SICOT J. 2023;9:19. doi: 10.1051/sicotj/2023015. Epub 2023 Jun 23. SICOT J. 2023. PMID: 37350673 Free PMC article.
-
A Systemic Review of Adolescent Supracondylar Fractures: What Is the Surgical Treatment, Open Reduction With Internal Fixation (ORIF) or Closed Reduction With Percutaneous Pinning (CRPP)?Cureus. 2024 Apr 12;16(4):e58123. doi: 10.7759/cureus.58123. eCollection 2024 Apr. Cureus. 2024. PMID: 38741793 Free PMC article. Review.
-
Comparative Analysis of Open Reduction Internal Fixation and Closed Reduction Percutaneous Pinning of Hand Fractures: Single Academic Center Retrospective Review.Ann Plast Surg. 2021 Jun 1;86(6S Suppl 5):S470-S472. doi: 10.1097/SAP.0000000000002877. Ann Plast Surg. 2021. PMID: 34100802 Review.
References
-
- Eltorai A EM, Durand W M, Haglin J M, Rubin L E, Weiss A C, Daniels A H. Trends in Medicare reimbursement for orthopedic procedures: 2000 to 2016. Orthopedics. 2018;41(02):95–102. - PubMed
-
- Malik A T, Kopechek K J, Bishop J Y, Cvetanovich G L, Khan S N, Neviaser A S. Declining trends in Medicare physician reimbursements for shoulder surgery from 2002 to 2018. J Shoulder Elbow Surg. 2020;29(12):e451–e461. - PubMed
-
- Nayar S K, Wollstein A, Sullivan B Tet al.Are we working harder for less pay? A survey of Medicare reimbursement for hand and upper extremity surgeryPlast Reconstr Surg2022 - PubMed
-
- Rupp M, Cambon-Binder A, Alt V, Feron J M. Is percutaneous pinning an outdated technique for distal radius fractures? Injury. 2019;50 01:S30–S35. - PubMed
LinkOut - more resources
Full Text Sources