

Incident pulmonary hypertension in 13 488 cases investigated with repeat echocardiography: a clinical cohort study
- PMID: 37701368
- PMCID: PMC10493707
- DOI: 10.1183/23120541.00082-2023
Incident pulmonary hypertension in 13 488 cases investigated with repeat echocardiography: a clinical cohort study
Abstract
Background: We addressed the paucity of data describing the characteristics and natural history of incident pulmonary hypertension.
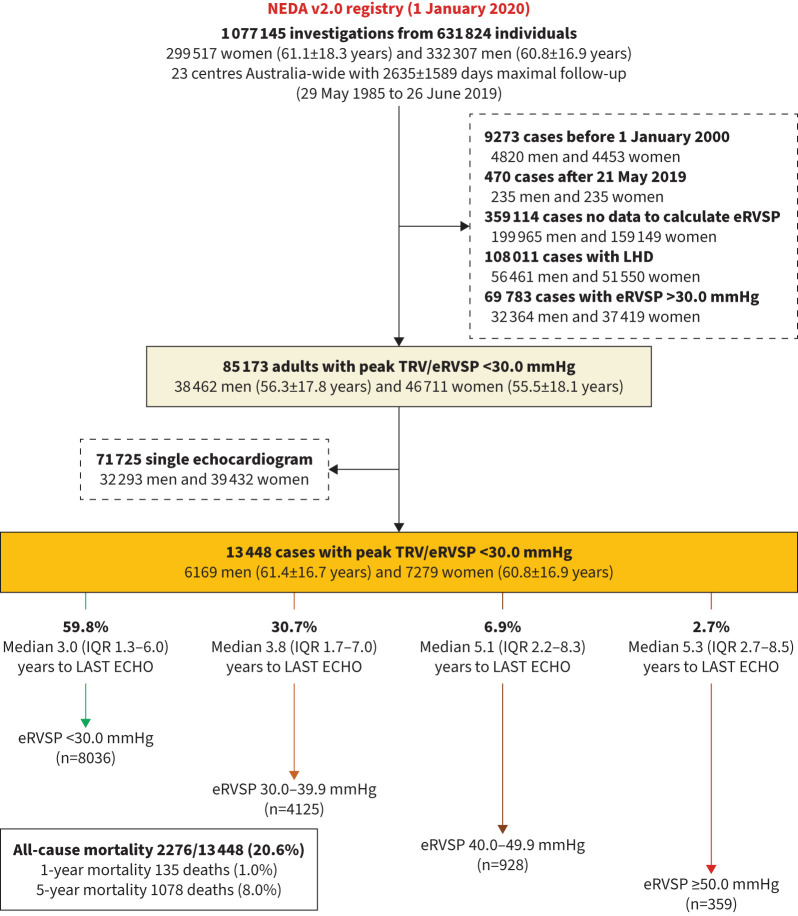
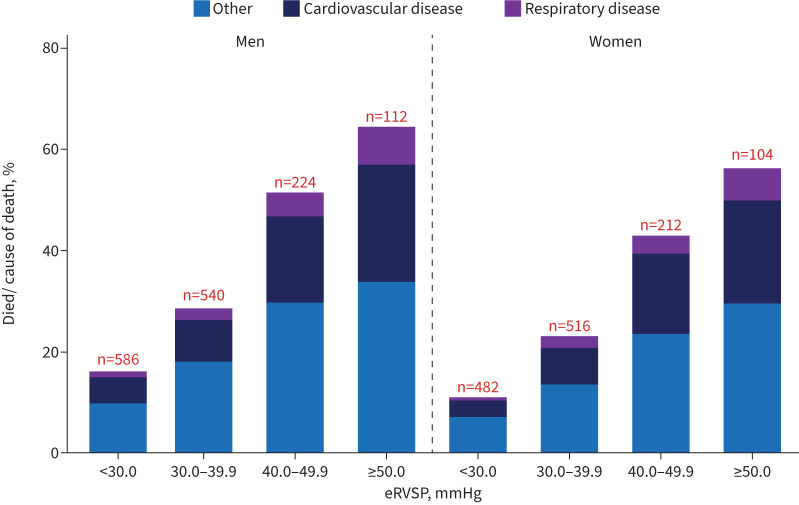
Methods: Adults (n=13 448) undergoing routine echocardiography without initial evidence of pulmonary hypertension (estimated right ventricular systolic pressure, eRVSP <30.0 mmHg) or left heart disease were studied. Incident pulmonary hypertension (eRVSP ≥30.0 mmHg) was detected on repeat echocardiogram a median of 4.1 years apart. Mortality was examined according to increasing eRVSP levels (30.0-39.9, 40.0-49.9 and ≥50.0 mmHg) indicative of mild-to-severe pulmonary hypertension.
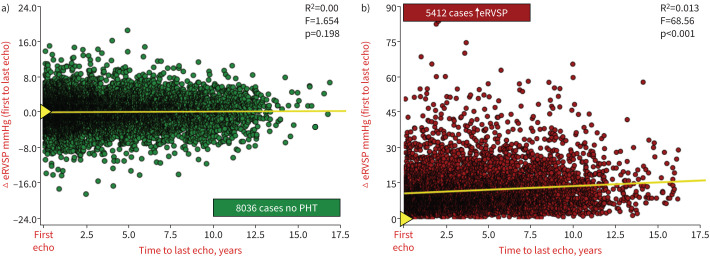
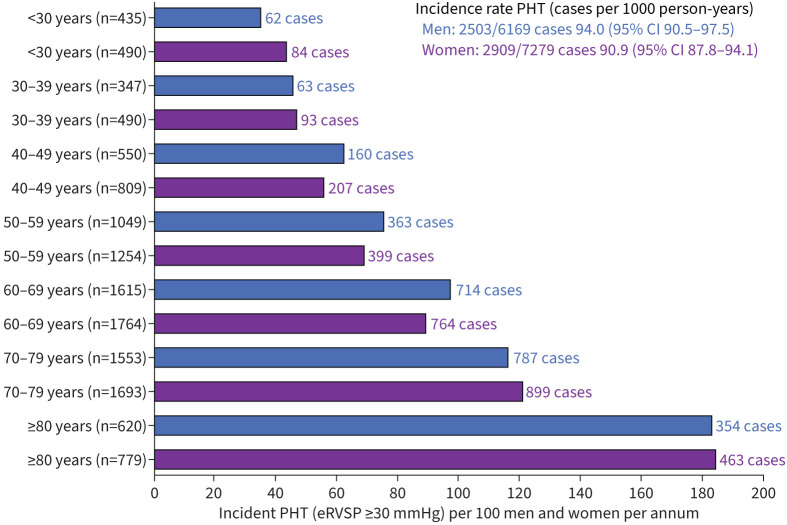
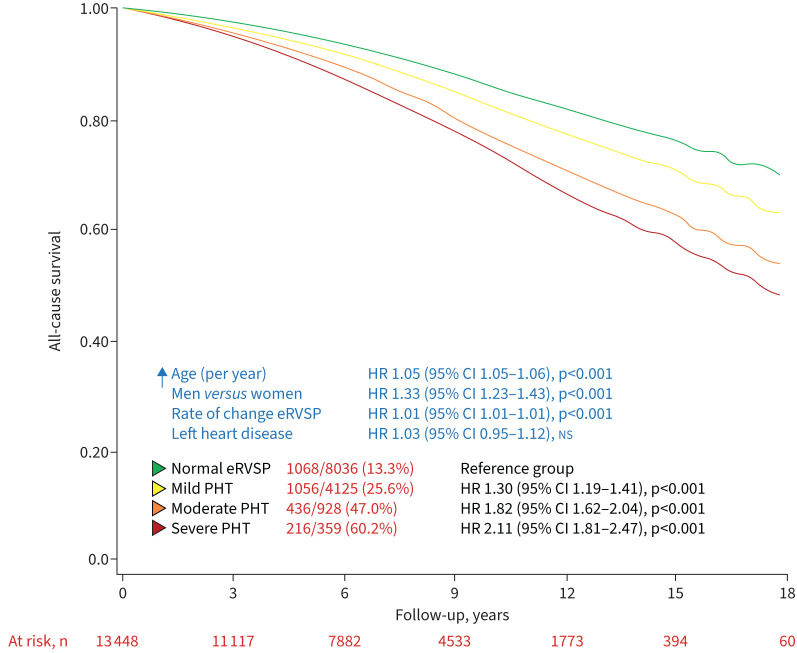
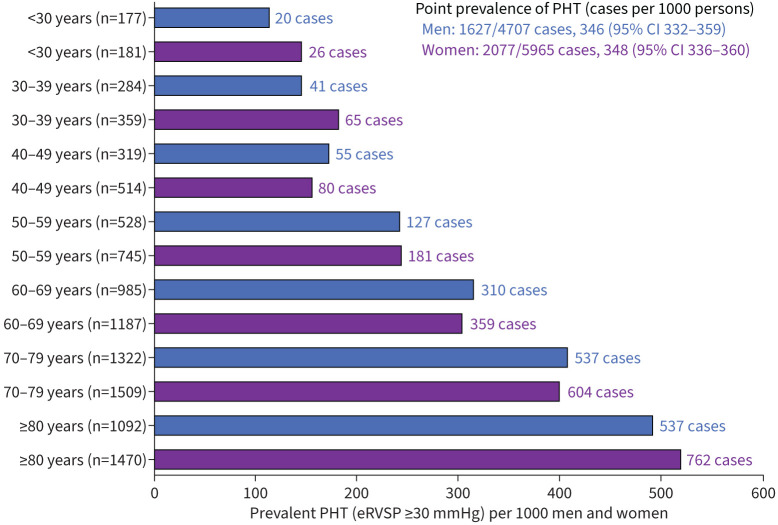
Results: A total of 6169 men (45.9%, aged 61.4±16.7 years) and 7279 women (60.8±16.9 years) without evidence of pulmonary hypertension were identified (first echocardiogram). Subsequently, 5412 (40.2%) developed evidence of pulmonary hypertension, comprising 4125 (30.7%), 928 (6.9%) and 359 (2.7%) cases with an eRVSP of 30.0-39.9 mmHg, 40.0-49.9 mmHg and ≥50.0 mmHg, respectively (incidence 94.0 and 90.9 cases per 1000 men and women, respectively, per year). Median (interquartile range) eRVSP increased by +0.0 (-2.27 to +2.67) mmHg and +30.68 (+26.03 to +37.31) mmHg among those with eRVSP <30.0 mmHg versus ≥50.0 mmHg. During a median 8.1 years of follow-up, 2776 (20.6%) died from all causes. Compared to those with eRVSP <30.0 mmHg, the adjusted risk of all-cause mortality was 1.30-fold higher in 30.0-39.9 mmHg, 1.82-fold higher in 40.0-49.9 mmHg and 2.11-fold higher in ≥50.0 mmHg groups (all p<0.001).
Conclusions: New-onset pulmonary hypertension, as indicated by elevated eRVSP, is a common finding among older patients without left heart disease followed-up with echocardiography. This phenomenon is associated with an increased morality risk even among those with mildly elevated eRVSP.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: S. Stewart reports grants or contracts from NHMRC Australia, outside the submitted work; consulting fees from NEDA, outside the submitted work; and honoraria for presentations from Novartis Pharmaceuticals, outside the submitted work. Conflict of interest: D. Playford reports support for the present manuscript received from Johnson & Johnson. Conflict of interest: G.A. Strange reports support for the present manuscript received from Johnson & Johnson. Conflict of interest: The remaining authors have nothing to disclose.
Figures
Similar articles
-
The Relationship between Pulmonary Artery Pressure and Mortality in Type 2 Diabetes: A Fremantle Diabetes Study Phase II and National Echocardiographic Database of Australia Data Linkage Study.J Clin Med. 2023 Dec 14;12(24):7685. doi: 10.3390/jcm12247685. J Clin Med. 2023. PMID: 38137754 Free PMC article.
-
Threshold of Pulmonary Hypertension Associated With Increased Mortality.J Am Coll Cardiol. 2019 Jun 4;73(21):2660-2672. doi: 10.1016/j.jacc.2019.03.482. J Am Coll Cardiol. 2019. PMID: 31146810
-
Prevalence of pulmonary hypertension in aortic regurgitation and its influence on outcomes.Heart. 2023 Aug 11;109(17):1310-1318. doi: 10.1136/heartjnl-2022-322187. Heart. 2023. PMID: 37012044
-
Prevalence, Incidence and Associates of Pulmonary Hypertension Complicating Type 2 Diabetes: Insights from the Fremantle Diabetes Study Phase 2 and National Echocardiographic Database of Australia.J Clin Med. 2021 Sep 29;10(19):4503. doi: 10.3390/jcm10194503. J Clin Med. 2021. PMID: 34640520 Free PMC article.
-
Prevalence of pulmonary hypertension in mitral regurgitation and its influence on outcomes.Open Heart. 2023 Jun;10(1):e002268. doi: 10.1136/openhrt-2023-002268. Open Heart. 2023. PMID: 37280015 Free PMC article.
Cited by
-
Incidence of Pulmonary Hypertension in the Echocardiography Referral Population.Ann Am Thorac Soc. 2025 May;22(5):679-688. doi: 10.1513/AnnalsATS.202407-716OC. Ann Am Thorac Soc. 2025. PMID: 39680898
-
Global distribution of prognostically significant pulmonary pressure indicative of pulmonary hypertension.J Glob Health. 2025 Mar 21;15:04098. doi: 10.7189/jogh.15.04098. J Glob Health. 2025. PMID: 40114580 Free PMC article.
-
Prognostic Value of Pulmonary Hypertension as an Incidental Finding Detected by Echocardiography in Patients Without Known Cardiovascular or Pulmonary Diseases.J Clin Med. 2025 Jul 16;14(14):5044. doi: 10.3390/jcm14145044. J Clin Med. 2025. PMID: 40725734 Free PMC article.
References
LinkOut - more resources
Full Text Sources