

Multimodality imaging of mediastinal masses and mimics
- PMID: 37701642
- PMCID: PMC10493620
- DOI: 10.21037/med-22-53
Multimodality imaging of mediastinal masses and mimics
Abstract
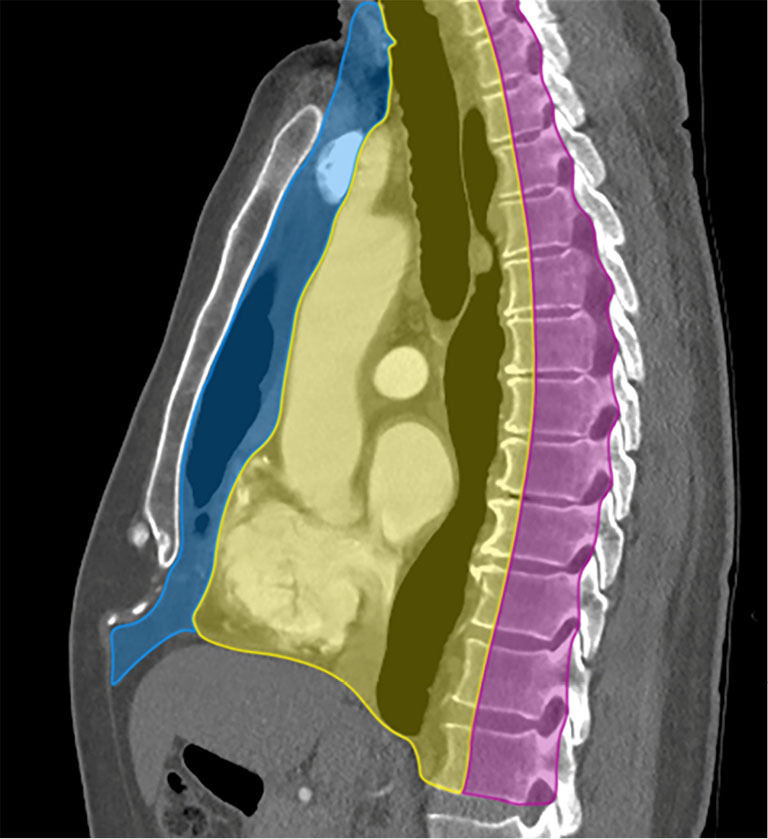
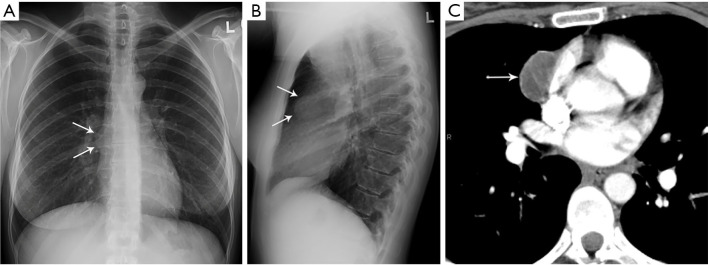
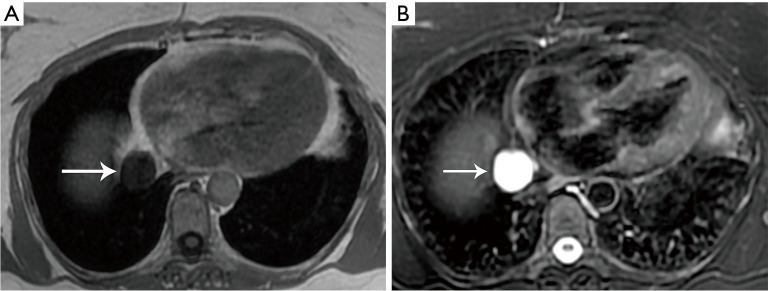
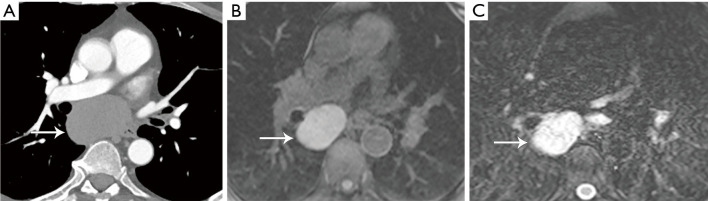
A wide variety of neoplastic and nonneoplastic conditions occur in the mediastinum. Imaging plays a central role in the evaluation of mediastinal pathologies and their mimics. Localization of a mediastinal lesion to a compartment and characterization of morphology, density/signal intensity, enhancement, and mass effect on neighboring structures can help narrow the differentials. The International Thymic Malignancy Interest Group (ITMIG) established a cross-sectional imaging-derived and anatomy-based classification system for mediastinal compartments, comprising the prevascular (anterior), visceral (middle), and paravertebral (posterior) compartments. Cross-sectional imaging is integral in the evaluation of mediastinal lesions. Computed tomography (CT) and magnetic resonance imaging (MRI) are useful to characterize mediastinal lesions detected on radiography. Advantages of CT include its widespread availability, fast acquisition time, relatively low cost, and ability to detect calcium. Advantages of MRI include the lack of radiation exposure, superior soft tissue contrast resolution to detect invasion of the mass across tissue planes, including the chest wall and diaphragm, involvement of neurovascular structures, and the potential for dynamic sequences during free-breathing or cinematic cardiac gating to assess motion of the mass relative to adjacent structures. MRI is superior to CT in the differentiation of cystic from solid lesions and in the detection of fat to differentiate thymic hyperplasia from thymic malignancy.
Keywords: Mediastinal compartments; computed tomography (CT); magnetic resonance imaging (MRI); mediastinal mass.
2023 Mediastinum. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://med.amegroups.com/article/view/10.21037/med-22-53/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Diagnostic approach to the anterior/prevascular mediastinum for radiologists.Mediastinum. 2019 May 27;3:18. doi: 10.21037/med.2018.12.03. eCollection 2019. Mediastinum. 2019. PMID: 35118246 Free PMC article. Review.
-
Approach to the prevascular mass.Mediastinum. 2019 May 8;3:17. doi: 10.21037/med.2019.04.05. eCollection 2019. Mediastinum. 2019. PMID: 35118245 Free PMC article. Review.
-
MR Imaging of Mediastinal Masses.Top Magn Reson Imaging. 2017 Aug;26(4):153-165. doi: 10.1097/RMR.0000000000000134. Top Magn Reson Imaging. 2017. PMID: 28777164 Review.
-
[Mediastinum-new compartment classification].Radiologie (Heidelb). 2023 Mar;63(3):154-159. doi: 10.1007/s00117-023-01115-w. Epub 2023 Jan 30. Radiologie (Heidelb). 2023. PMID: 36715717 Review. German.
-
Pediatric mediastinal masses.Pediatr Radiol. 2022 Sep;52(10):1935-1947. doi: 10.1007/s00247-022-05409-4. Epub 2022 Jun 8. Pediatr Radiol. 2022. PMID: 35674800 Review.
Cited by
-
Minimally Invasive Sampling of Mediastinal Lesions.Life (Basel). 2024 Oct 11;14(10):1291. doi: 10.3390/life14101291. Life (Basel). 2024. PMID: 39459591 Free PMC article. Review.
-
Diagnostic and Therapeutic Challenges of Cardiac Metastasis in Advanced Malignancies: A Case Series and Literature Review.Case Rep Oncol Med. 2025 May 24;2025:7374561. doi: 10.1155/crom/7374561. eCollection 2025. Case Rep Oncol Med. 2025. PMID: 40453961 Free PMC article.
-
Cine-MRI and T1TSE Sequence for Mediastinal Mass.Cancers (Basel). 2024 Sep 15;16(18):3162. doi: 10.3390/cancers16183162. Cancers (Basel). 2024. PMID: 39335134 Free PMC article.
-
A diagnostic approach to mediastinal masses in clinical practice.BJR Open. 2025 May 8;7(1):tzaf009. doi: 10.1093/bjro/tzaf009. eCollection 2025 Jan. BJR Open. 2025. PMID: 40641909 Free PMC article. Review.
-
The combination of maximum standardized uptake value and clinical parameters for improving the accuracy in distinguishing primary mediastinal lymphomas from thymic epithelial tumors.Quant Imaging Med Surg. 2024 Feb 1;14(2):1944-1956. doi: 10.21037/qims-23-496. Epub 2024 Jan 5. Quant Imaging Med Surg. 2024. PMID: 38415117 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources