

A Dedicated Simulator Training Curriculum Improves Resident Performance in Surgical Management of Pediatric Supracondylar Humerus Fractures
- PMID: 37701678
- PMCID: PMC10489481
- DOI: 10.2106/JBJS.OA.23.00031
A Dedicated Simulator Training Curriculum Improves Resident Performance in Surgical Management of Pediatric Supracondylar Humerus Fractures
Abstract
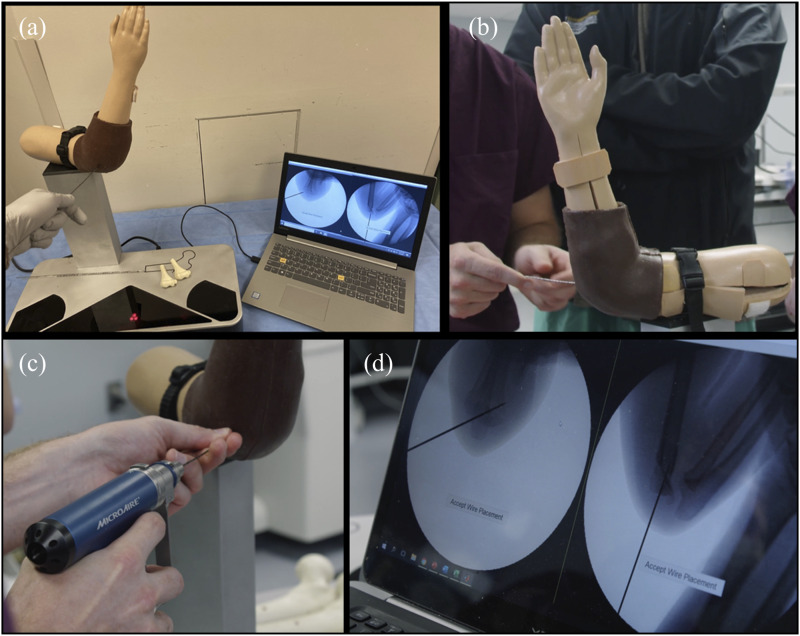
Background: The primary goal of including simulation in residency training is to improve technical skills while working outside of the operating room. Such simulation-related skill improvements have seldom been measured in the operating room. This is largely because uncontrolled variables, such as injury severity, patient comorbidity, and anatomical variation, can bias evaluation of an operating surgeon's skill. In this study, performance during the wire navigation phase of pediatric supracondylar humerus fracture fixation was quantitatively compared between 2 groups of orthopaedic residents: a standard training group consisting of residents who participated in a single simulator session of wire navigation training and an expanded training group consisting of residents who participated in a dedicated multifaceted wire navigation simulation training curriculum.
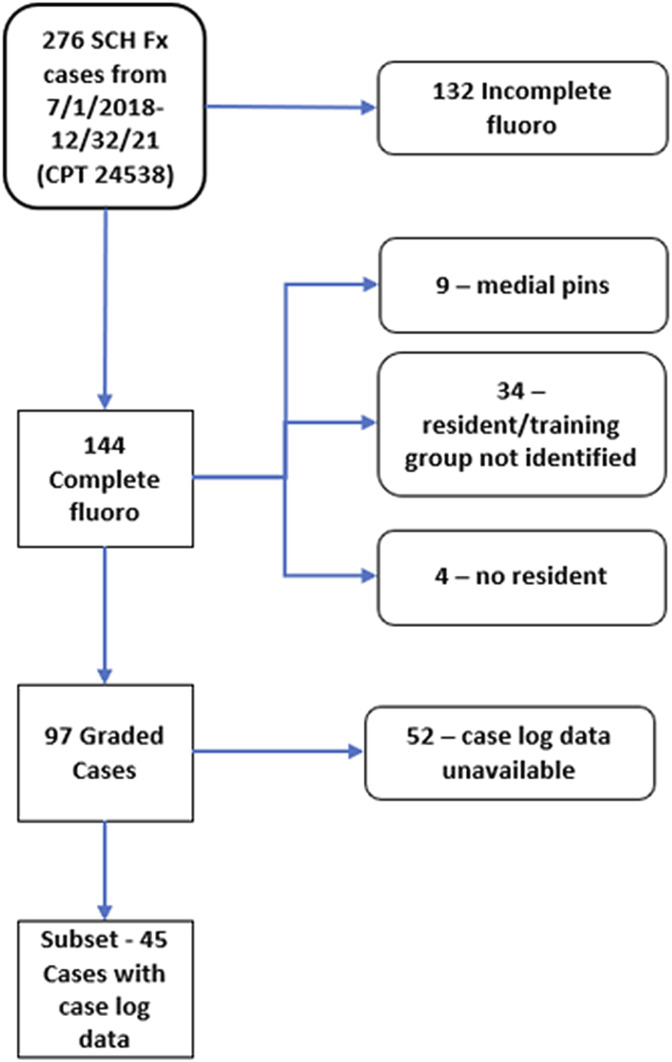
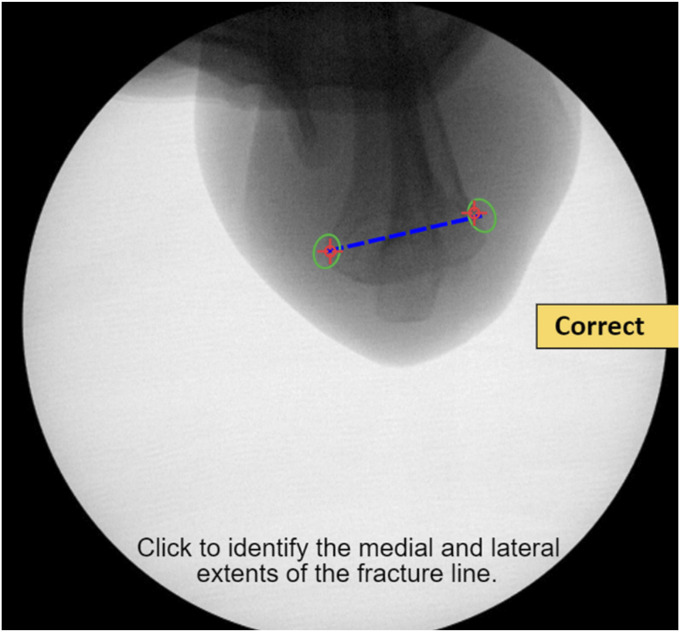
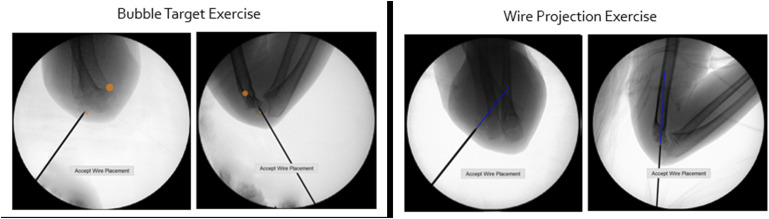
Methods: To evaluate performance in the operating room, the full sequence of fluoroscopic images collected during wire navigation was quantitatively analyzed. Objective performance metrics included number of fluoroscopic images acquired, duration from placement of the first wire to that of the final wire, and wire spread at the level of the fracture. These metrics were measured from 97 pediatric supracondylar humerus fracture pinning surgeries performed by 28 different orthopaedic residents.
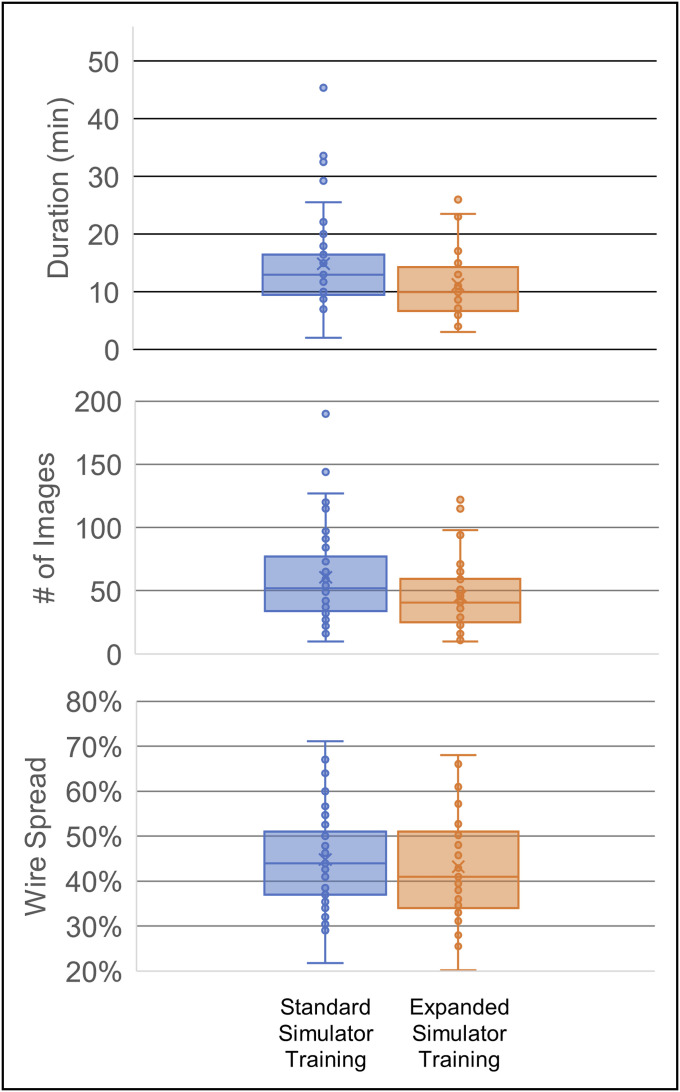
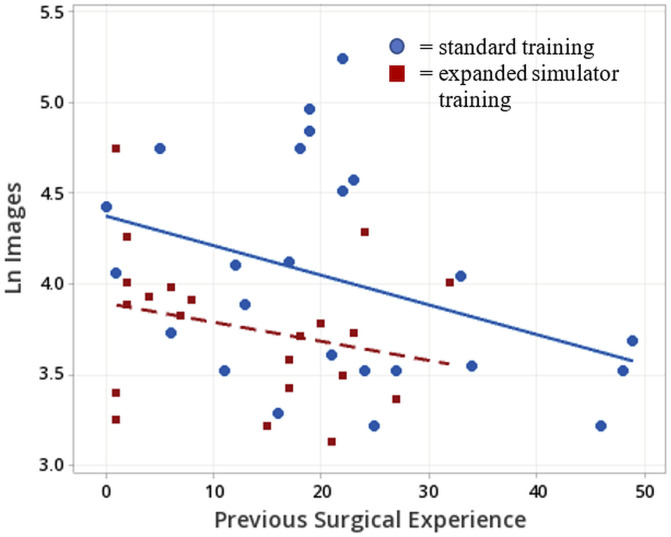
Results: No differences were observed between the groups for wire spread in the final fluoroscopic images (t(94) = 0.75, p = 0.45), an important clinical objective of the surgery. Residents who received the expanded simulator training used significantly fewer fluoroscopic images (mean of 46 vs. 61 images, t(85) = 2.25, p < 0.03) and required less time from first to final wire placement (mean of 11.2 vs. 14.9 minutes, t(83) = 2.53, p = 0.013) than the standard training group. A post hoc review of Accreditation Council for Graduate Medical Education case logs for 24 cases from the standard training group and for 21 cases from the expanded training group indicated that, at the time of surgeries, residents who received expanded training had completed fewer comparable cases than residents in the standard training group (mean of 13 vs. 21, t(42) = 2.40 p = 0.02). Further regression analysis indicated that the expanded simulator training produced an effect comparable with that associated with completing 10.5 similar surgical case experiences.
Conclusions: This study demonstrates that training on a wire navigation simulator can lead to improved performance in the operating room on a critical skill for all orthopaedic residents. By taking fewer images and less time while maintaining sufficient pin spread, simulator-trained residents were objectively measured to have improved performance in comparison with residents who had not participated in the pediatric elbow simulator curriculum.
Clinical relevance: As programs aim to provide safe and effective training for critical orthopaedic skills such as pinning a pediatric elbow, this study demonstrates a simulator curriculum that has demonstrated the transfer of skill from a learning environment to the operating room.
Copyright © 2023 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Conflict of interest statement
Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSOA/A546).
Figures
Similar articles
-
Surgical Skill Can be Objectively Measured From Fluoroscopic Images Using a Novel Image-based Decision Error Analysis (IDEA) Score.Clin Orthop Relat Res. 2021 Jun 1;479(6):1386-1394. doi: 10.1097/CORR.0000000000001623. Clin Orthop Relat Res. 2021. PMID: 33399401 Free PMC article.
-
Do Skills Acquired from Training with a Wire Navigation Simulator Transfer to a Mock Operating Room Environment?Clin Orthop Relat Res. 2019 Oct;477(10):2189-2198. doi: 10.1097/CORR.0000000000000799. Clin Orthop Relat Res. 2019. PMID: 31135546 Free PMC article.
-
Establishing Construct Validity of a Novel Simulator for Guide Wire Navigation in Antegrade Femoral Intramedullary Nailing.Iowa Orthop J. 2023;43(1):31-35. Iowa Orthop J. 2023. PMID: 37383869 Free PMC article.
-
A Novel Low-Cost Surgical Simulation Tool for Pinning Supracondylar Humerus Fractures.J Pediatr Orthop. 2020 May/Jun;40(5):e317-e321. doi: 10.1097/BPO.0000000000001460. J Pediatr Orthop. 2020. PMID: 31633592
-
Effectiveness of a microvascular surgery training curriculum for orthopaedic surgery residents.J Bone Joint Surg Am. 2015 Jun 3;97(11):950-5. doi: 10.2106/JBJS.N.00854. J Bone Joint Surg Am. 2015. PMID: 26041858 Review.
Cited by
-
Objective Fluoroscopic Image-Based Assessment of Intraoperative Wire Navigation Skill Agrees with Subjective Expert Opinion.Iowa Orthop J. 2025;45(1):49-59. Iowa Orthop J. 2025. PMID: 40606727 Free PMC article.
-
Opportunity to Perform - Should Simulation-Based Surgical Training be Provided on Demand or on Supply?J Med Educ Curric Dev. 2023 Dec 6;10:23821205231219429. doi: 10.1177/23821205231219429. eCollection 2023 Jan-Dec. J Med Educ Curric Dev. 2023. PMID: 38075444 Free PMC article.
-
A Surgical Skills Rotation for Mid-Level Residents.JB JS Open Access. 2024 Jul 17;9(3):e24.00036. doi: 10.2106/JBJS.OA.24.00036. eCollection 2024 Jul-Sep. JB JS Open Access. 2024. PMID: 39021675 Free PMC article. Review.
References
-
- Aggarwal R, Mytton OT, Derbrew M, Hananel D, Heydenburg M, Issenberg B, MacAulay C, Mancini ME, Morimoto T, Soper N, Ziv A, Reznick R. Training and simulation for patient safety. Qual Saf Health Care. 2010;19(suppl 2):i34-43. - PubMed
-
- Nzeako O, Back D. Learning curves in arthroplasty in orthopedic trainees. J Surg Educ. 2016;73:689-93. - PubMed
-
- Marston RA, Cobb AG, Bentley G. Stanmore compared with Charnley total hip replacement. A prospective study of 413 arthroplasties. J Bone Joint Surg Br. 1996;78:178-84. - PubMed
-
- Inaba K, Recinos G, Teixeira PG, Barmparas G, Talving P, Salim A, Brown C, Rhee P, Demetriades D. Complications and death at the start of the new academic year: is there a July phenomenon? J Trauma Acute Care Surg. 2010;68:19-22. - PubMed
-
- Bagsby D, Loder R, Myung K. Operative intervention of supracondylar humerus fractures more complicated in July: analysis of the July effect. J Pediatr Orthop. 2017;37:254-7. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials