

Goldilocks principle of minimally invasive surgery for gastric subepithelial tumors
- PMID: 37701681
- PMCID: PMC10494604
- DOI: 10.4240/wjgs.v15.i8.1629
Goldilocks principle of minimally invasive surgery for gastric subepithelial tumors
Abstract
Background: Minimally invasive surgery had been tailored to individual cases of gastric subepithelial tumors (SETs) after comparing the clinical outcomes of endoscopic resection (ER), laparoscopic resection (LR), and hybrid methods.
Aim: To study the use of Goldilocks principle to determine the best form of minimally invasive surgery for gastric SETs.
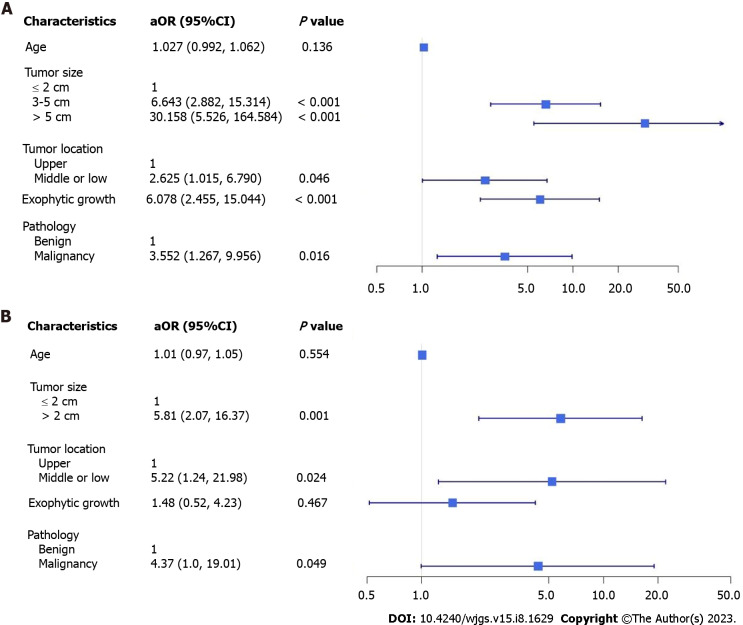
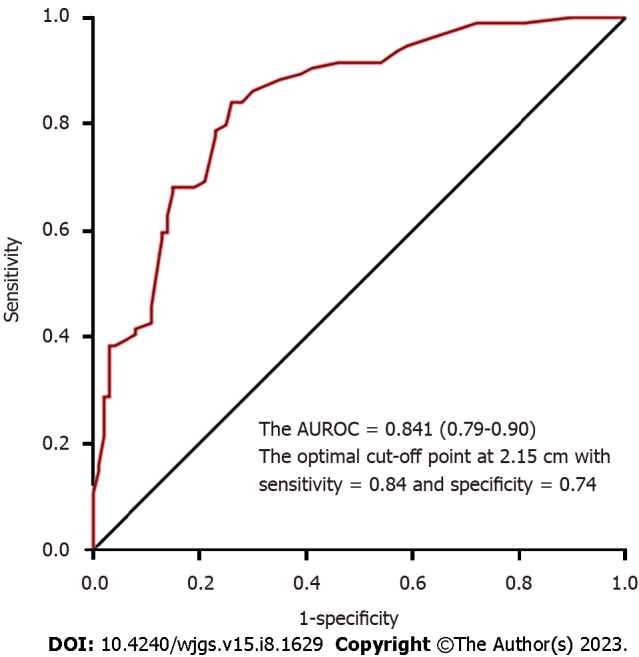
Methods: In this retrospective study, 194 patients of gastric SETs with high probability of surgical intervention were included. All patients underwent tumor resection in the operating theater between January 2013 and December 2021. The patients were divided into two groups, ER or LR, according to the tumor characteristics and the initial intent of intervention. Few patients in the ER group required further backup laparoscopic surgery after an incomplete ER. The patients who had converted open surgery were excluded. A logistic regression model was used to assess the associations between patient characteristics and the likelihood of a treatment strategy. The area under the curve was used to assess the discriminative ability of tumor size and Youden's index to determine the optimal cut-off tumor size.
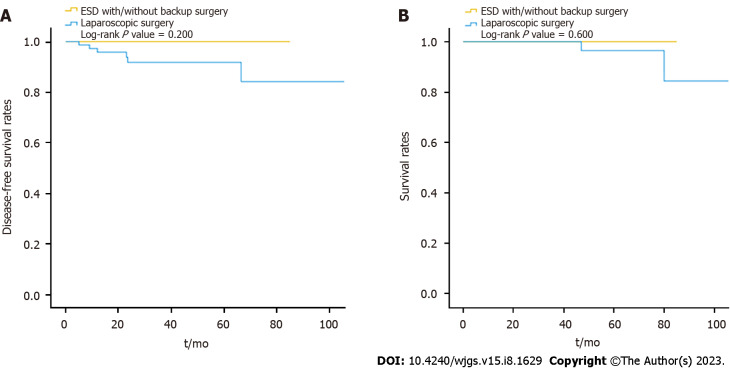
Results: One-hundred ninety-four patients (100 in the ER group and 94 in the LR group) underwent tumor resection in the operating theater. In the ER group, 27 patients required backup laparoscopic surgery after an incomplete ER. The patients in the ER group had small tumor sizes and shorter procedure durations while the patients in the LR group had large tumor sizes, exophytic growth, malignancy, and tumors that were more often located in the middle or lower third of the stomach. Both groups had similar durations of hospital stays and a similar rate of major postoperative complications. The patients in the ER group who underwent backup surgery required longer procedures (56.4 min) and prolonged stays (2 d) compared to the patients in the LR group without the increased rate of major postoperative complications. The optimal cut-off point for the tumor size for laparoscopic surgery was 2.15 cm.
Conclusion: Multidisciplinary teamwork leads to the adoption of different strategies to yield efficient clinical outcomes according to the tumor characteristics.
Keywords: Endoscopic resection; Gastric subepithelial tumors; Laparoscopic resection; Tumor size.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Endoscopic Resection for Gastric Subepithelial Tumor with Backup Laparoscopic Surgery: Description of a Single-Center Experience.J Clin Med. 2021 Sep 27;10(19):4423. doi: 10.3390/jcm10194423. J Clin Med. 2021. PMID: 34640444 Free PMC article.
-
Comparison between endoscopic and laparoscopic removal of gastric submucosal tumor.Dig Endosc. 2018 Apr;30 Suppl 1:7-16. doi: 10.1111/den.13010. Dig Endosc. 2018. PMID: 29658656
-
Simple and Reliable Method for Gastric Subepithelial Tumor Localization Using Endoscopic Tattooing before Totally Laparoscopic Resection.J Pers Med. 2021 Aug 28;11(9):855. doi: 10.3390/jpm11090855. J Pers Med. 2021. PMID: 34575632 Free PMC article.
-
Laparoscopy-assisted endoscopic full-thickness resection for gastric subepithelial tumors originated from the muscularis propria layer: a pilot study with literature review.Scand J Gastroenterol. 2017 Mar;52(3):257-263. doi: 10.1080/00365521.2016.1230778. Epub 2016 Dec 20. Scand J Gastroenterol. 2017. PMID: 27996335 Review.
-
Safety and efficiency of endoscopic resection versus laparoscopic resection in gastric gastrointestinal stromal tumours: A systematic review and meta-analysis.Eur J Surg Oncol. 2020 Apr;46(4 Pt A):667-674. doi: 10.1016/j.ejso.2019.10.030. Epub 2019 Dec 13. Eur J Surg Oncol. 2020. PMID: 31864827
Cited by
-
Feasibility and safety of endoscopic full-thickness resection of large gastric subepithelial lesions outside the operating room: 10 years of experience in a large tertiary hospital in China.Surg Endosc. 2025 Aug 8. doi: 10.1007/s00464-025-11997-7. Online ahead of print. Surg Endosc. 2025. PMID: 40779132
-
Endoscopic Resection Versus Laparoscopic Resection for Gastric Submucosal Tumors: A Systematic Review and Meta-Analysis of Safety and Efficacy.Asian J Endosc Surg. 2025 Jan-Dec;18(1):e70104. doi: 10.1111/ases.70104. Asian J Endosc Surg. 2025. PMID: 40555559 Free PMC article.
References
-
- Hwang JH, Rulyak SD, Kimmey MB American Gastroenterological Association Institute. American Gastroenterological Association Institute technical review on the management of gastric subepithelial masses. Gastroenterology. 2006;130:2217–2228. - PubMed
-
- Casali PG, Abecassis N, Aro HT, Bauer S, Biagini R, Bielack S, Bonvalot S, Boukovinas I, Bovee JVMG, Brodowicz T, Broto JM, Buonadonna A, De Álava E, Dei Tos AP, Del Muro XG, Dileo P, Eriksson M, Fedenko A, Ferraresi V, Ferrari A, Ferrari S, Frezza AM, Gasperoni S, Gelderblom H, Gil T, Grignani G, Gronchi A, Haas RL, Hassan B, Hohenberger P, Issels R, Joensuu H, Jones RL, Judson I, Jutte P, Kaal S, Kasper B, Kopeckova K, Krákorová DA, Le Cesne A, Lugowska I, Merimsky O, Montemurro M, Pantaleo MA, Piana R, Picci P, Piperno-Neumann S, Pousa AL, Reichardt P, Robinson MH, Rutkowski P, Safwat AA, Schöffski P, Sleijfer S, Stacchiotti S, Sundby Hall K, Unk M, Van Coevorden F, van der Graaf WTA, Whelan J, Wardelmann E, Zaikova O, Blay JY ESMO Guidelines Committee and EURACAN. Gastrointestinal stromal tumours: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv68–iv78. - PubMed
-
- von Mehren M, Kane JM, Bui MM, Choy E, Connelly M, Dry S, Ganjoo KN, George S, Gonzalez RJ, Heslin MJ, Homsi J, Keedy V, Kelly CM, Kim E, Liebner D, McCarter M, McGarry SV, Meyer C, Pappo AS, Parkes AM, Paz IB, Petersen IA, Poppe M, Riedel RF, Rubin B, Schuetze S, Shabason J, Sicklick JK, Spraker MB, Zimel M, Bergman MA, George GV. NCCN Guidelines Insights: Soft Tissue Sarcoma, Version 1.2021. J Natl Compr Canc Netw. 2020;18:1604–1612. - PubMed
LinkOut - more resources
Full Text Sources
