

Vascular complications of chronic pancreatitis and its management
- PMID: 37701688
- PMCID: PMC10494584
- DOI: 10.4240/wjgs.v15.i8.1574
Vascular complications of chronic pancreatitis and its management
Abstract
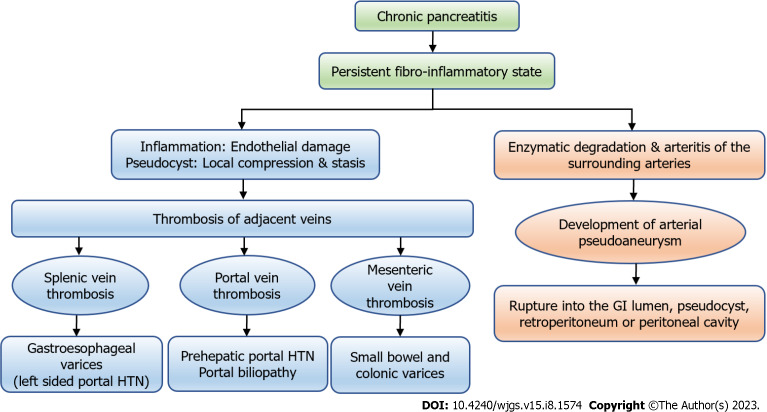
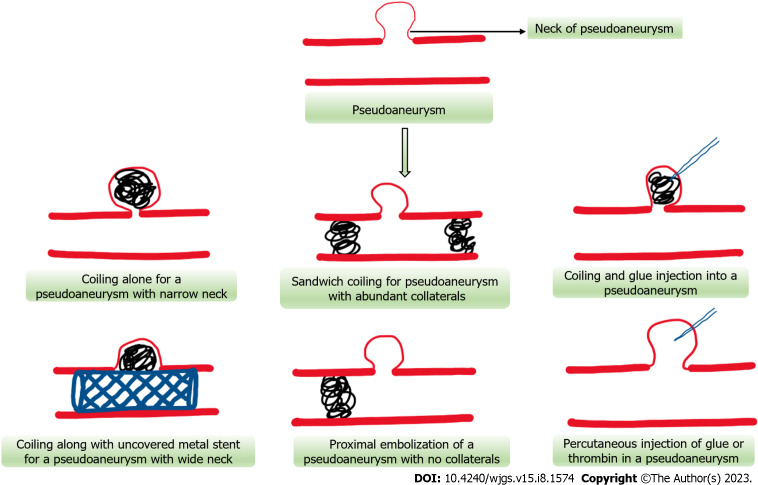
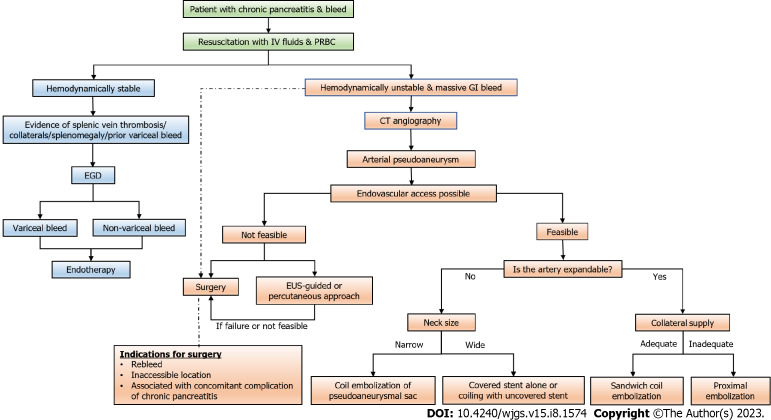
Chronic pancreatitis is a chronic fibro-inflammatory disorder of the pancreas, resulting in recurrent abdominal pain, diabetes mellitus, and malnutrition. It may lead to various other complications such as pseudocyst formation, benign biliary stricture, gastric outlet obstruction; and vascular complications like venous thrombosis, variceal and pseudoaneurysmal bleed. Development of varices is usually due to chronic venous thrombosis with collateral formation and variceal bleeding can easily be tackled by endoscopic therapy. Pseudoaneurysmal bleed can be catastrophic and requires radiological interventions including digital subtraction angiography followed by endovascular obliteration, or sometimes with a percutaneous or an endoscopic ultrasound-guided approach in technically difficult situations. Procedure-related bleed is usually venous and mostly managed conservatively. Procedure-related arterial bleed, however, may require radiological interventions.
Keywords: Chronic pancreatitis; Pseudoaneurysm; Varices; Vascular complications; Venous thrombosis.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
References
-
- Vege SS, Chari ST. Chronic Pancreatitis. N Engl J Med. 2022;386:869–878. - PubMed
-
- Agarwal S, Sharma S, Gunjan D, Singh N, Kaushal K, Poudel S, Anand A, Gopi S, Mohta S, Sonika U, Saraya A. Natural course of chronic pancreatitis and predictors of its progression. Pancreatology. 2020;20:347–355. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
