

Urinary Paraben Concentrations and Associations with the Periconceptional Urinary Metabolome: Untargeted and Targeted Metabolomics Analyses of Participants from the Early Pregnancy Study
- PMID: 37702489
- PMCID: PMC10498870
- DOI: 10.1289/EHP12125
Urinary Paraben Concentrations and Associations with the Periconceptional Urinary Metabolome: Untargeted and Targeted Metabolomics Analyses of Participants from the Early Pregnancy Study
Abstract
Background: Parabens, found in everyday items from personal care products to foods, are chemicals with endocrine-disrupting activity, which has been shown to influence reproductive function.
Objectives: This study investigated whether urinary concentrations of methylparaben, propylparaben, or butylparaben were associated with the urinary metabolome during the periconceptional period, a critical window for female reproductive function. Changes to the periconceptional urinary metabolome could provide insights into the mechanisms by which parabens could impact fertility.
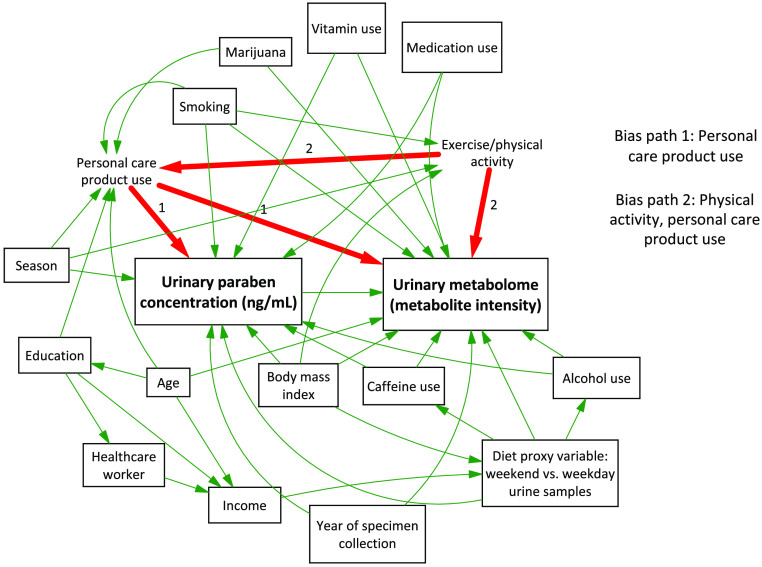
Methods: Urinary paraben concentrations were measured in paired pre- and postconception urine samples from 42 participants in the Early Pregnancy Study, a prospective cohort of 221 women attempting to conceive. We performed untargeted and targeted metabolomics analyses using ultrahigh-performance liquid chromatography quadrupole time-of-flight mass spectrometry. We used principal component analysis, orthogonal partial least-squares discriminant analysis, and permutation testing, coupled with univariate statistical analyses, to find metabolites associated with paraben concentration at the two time points. Potential confounders were identified with a directed acyclic graph and used to adjust results with multivariable linear regression. Metabolites were identified using fragmentation data.
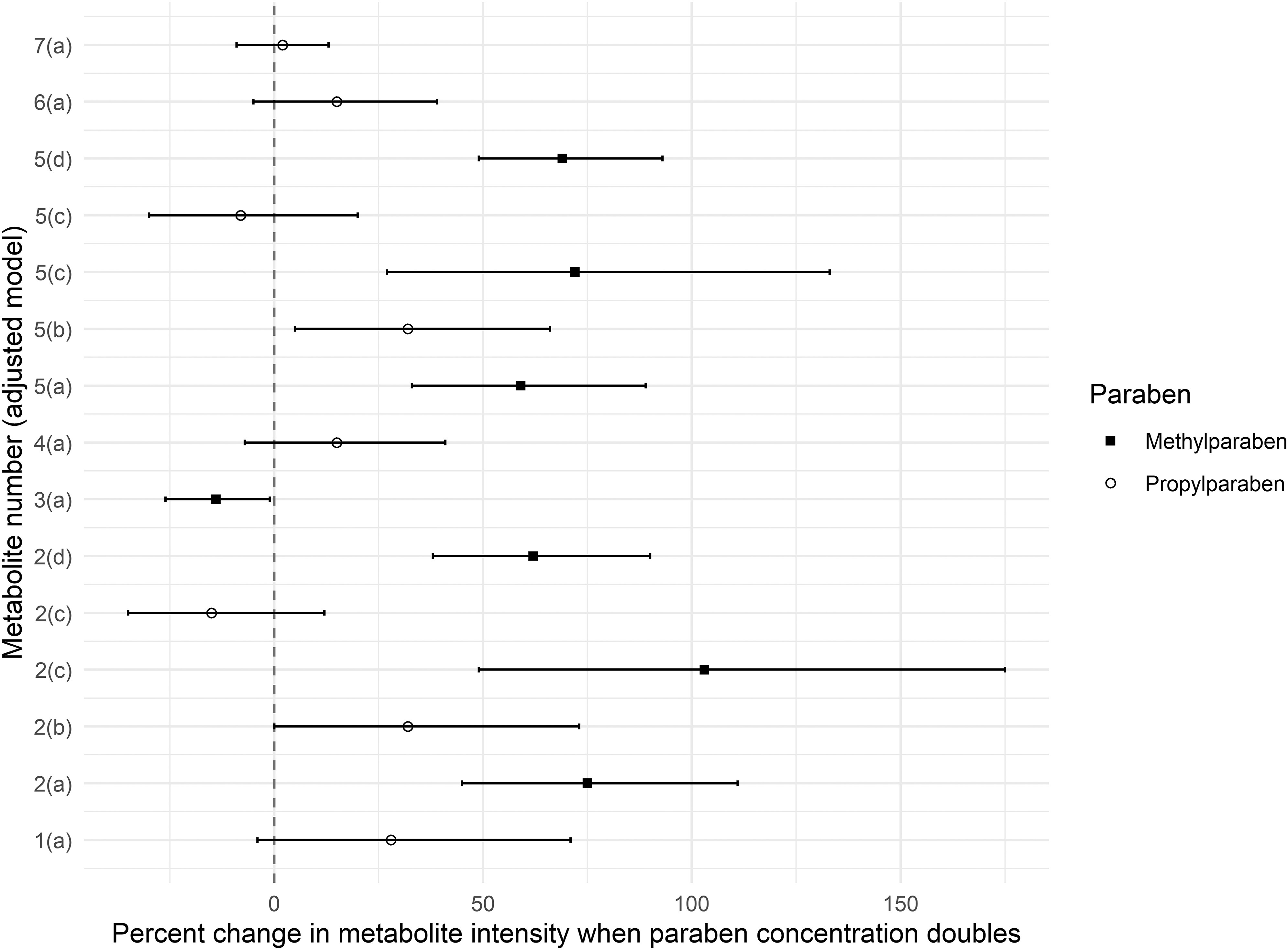
Results: Seven metabolites were associated with paraben concentration (variable importance to projection score , false discovery rate-corrected ). We identified four diet-related metabolites to the Metabolomics Standards Initiative (MSI) certainty of identification level 2, including metabolites from smoke flavoring, grapes, and olive oil. One metabolite was identified to the class level only (MSI level 3). Two metabolites were unidentified (MSI level 4). After adjustment, three metabolites remained associated with methylparaben and propylparaben, two of which were diet-related. No metabolomic markers of endocrine disruption were associated with paraben concentrations.
Discussion: This study identified novel relationships between urinary paraben concentrations and diet-related metabolites but not with metabolites on endocrine-disrupting pathways, as hypothesized. It demonstrates the feasibility of integrating untargeted metabolomics data with environmental exposure information and epidemiological adjustment for confounders. The findings underscore a potentially important connection between diet and paraben exposure, with applications to nutritional epidemiology and dietary exposure assessment. https://doi.org/10.1289/EHP12125.
Figures
References
-
- Meeker JD, Cantonwine DE, Rivera-González LO, Ferguson KK, Mukherjee B, Calafat AM, et al. 2013. Distribution, variability, and predictors of urinary concentrations of phenols and parabens among pregnant women in Puerto Rico. Environ Sci Technol 47(7):3439–3447, PMID: , 10.1021/es400510g. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources