

Economic Evaluation of Extended-Release Buprenorphine for Persons With Opioid Use Disorder
- PMID: 37703018
- PMCID: PMC10500382
- DOI: 10.1001/jamanetworkopen.2023.29583
Economic Evaluation of Extended-Release Buprenorphine for Persons With Opioid Use Disorder
Abstract
Importance: In 2017, the US Food and Drug Administration (FDA) approved a monthly injectable form of buprenorphine, extended-release buprenorphine; published data show that extended-release buprenorphine is effective compared with no treatment, but its current cost is higher and current retention is lower than that of transmucosal buprenorphine. Preliminary research suggests that extended-release buprenorphine may be an important addition to treatment options, but the cost-effectiveness of extended-release buprenorphine compared with transmucosal buprenorphine remains unclear.
Objective: To evaluate the cost-effectiveness of extended-release buprenorphine compared with transmucosal buprenorphine.
Design, setting, and participants: This economic evaluation used a state transition model starting in 2019 to simulate the lifetime of a closed cohort of individuals with OUD presenting for evaluation for opioid agonist treatment with buprenorphine. The data sources used to estimate model parameters included cohort studies, clinical trials, and administrative data. The model relied on pharmaceutical costs from the Federal Supply Schedule and health care utilization costs from published studies. Data were analyzed from September 2021 to January 2023.
Interventions: No treatment, treatment with transmucosal buprenorphine, or treatment with extended-release buprenorphine.
Main outcomes and measures: Mean lifetime costs per person, discounted quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratios (ICERs).
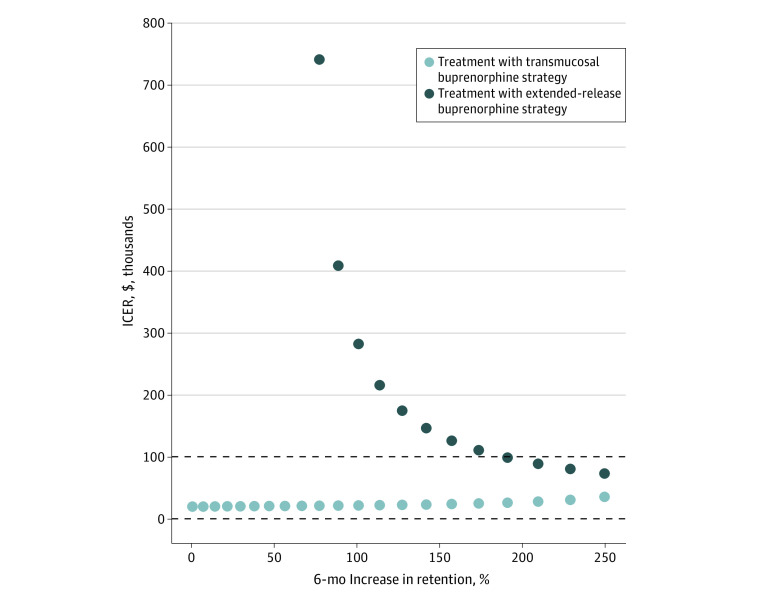
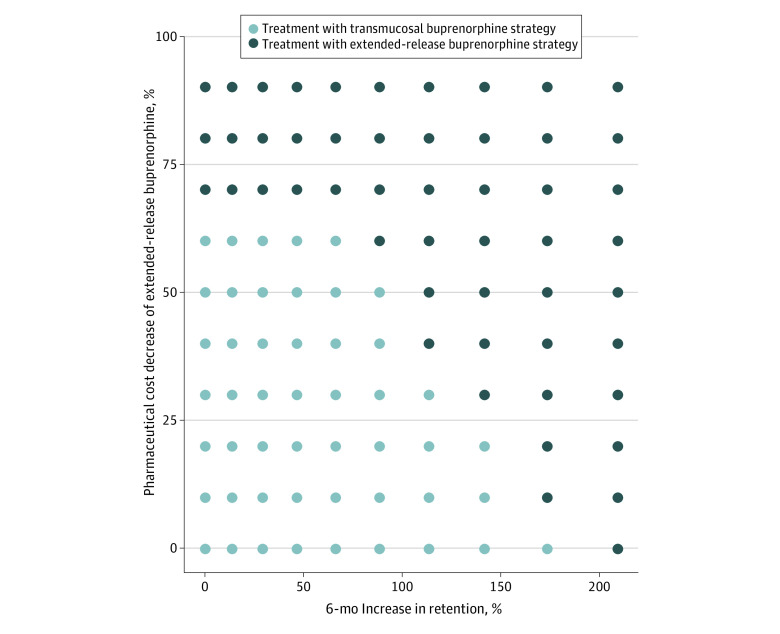
Results: The simulated cohort included 100 000 patients with OUD receiving (61% male; mean [SD] age, 38 [11] years) or not receiving medication treatment (58% male, mean [SD] age, 48 [18] years). Compared with no medication treatment, treatment with transmucosal buprenorphine yielded an ICER of $19 740 per QALY. Compared with treatment with transmucosal buprenorphine, treatment with extended-release buprenorphine yielded lower effectiveness by 0.03 QALYs per person at higher cost, suggesting that treatment with extended-release buprenorphine was dominated and not preferred. In probabilistic sensitivity analyses, treatment with transmucosal buprenorphine was the preferred strategy 60% of the time. Treatment with extended-release buprenorphine was cost-effective compared with treatment with transmucosal buprenorphine at a $100 000 per QALY willingness-to-pay threshold only after substantial changes in key parameters.
Conclusions and relevance: In this economic evaluation of extended-release buprenorphine compared with transmucosal buprenorphine for the treatment of OUD, extended-release buprenorphine was not associated with efficient allocation of limited resources when transmucosal buprenorphine was available. Future initiatives should aim to improve retention rates or decrease costs associated with extended-release buprenorphine.
Conflict of interest statement
Figures
Comment in
-
Challenges of Estimating the Value of Buprenorphine Injectables.JAMA Netw Open. 2023 Sep 5;6(9):e2329677. doi: 10.1001/jamanetworkopen.2023.29677. JAMA Netw Open. 2023. PMID: 37703021 No abstract available.
References
-
- CDC . Provisional drug overdose death counts. 2022. Accessed October 4, 2022. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
