

Association of Coronary Artery Calcium Detected by Routine Ungated CT Imaging With Cardiovascular Outcomes
- PMID: 37704309
- PMCID: PMC11009374
- DOI: 10.1016/j.jacc.2023.06.040
Association of Coronary Artery Calcium Detected by Routine Ungated CT Imaging With Cardiovascular Outcomes
Abstract
Background: Coronary artery calcium (CAC) is a strong predictor of cardiovascular events across all racial and ethnic groups. CAC can be quantified on nonelectrocardiography (ECG)-gated computed tomography (CT) performed for other reasons, allowing for opportunistic screening for subclinical atherosclerosis.
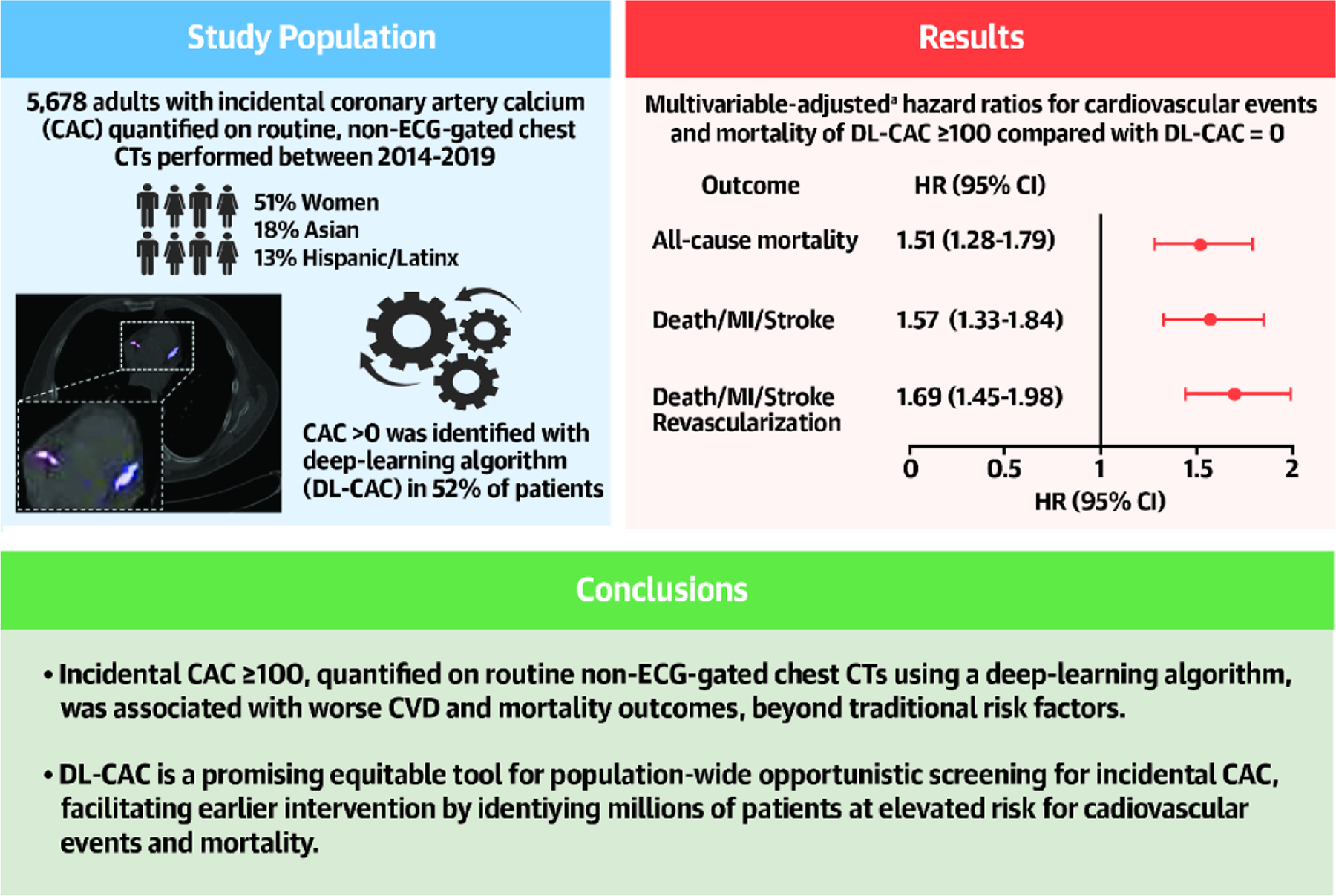
Objectives: The authors investigated whether incidental CAC quantified on routine non-ECG-gated CTs using a deep-learning (DL) algorithm provided cardiovascular risk stratification beyond traditional risk prediction methods.
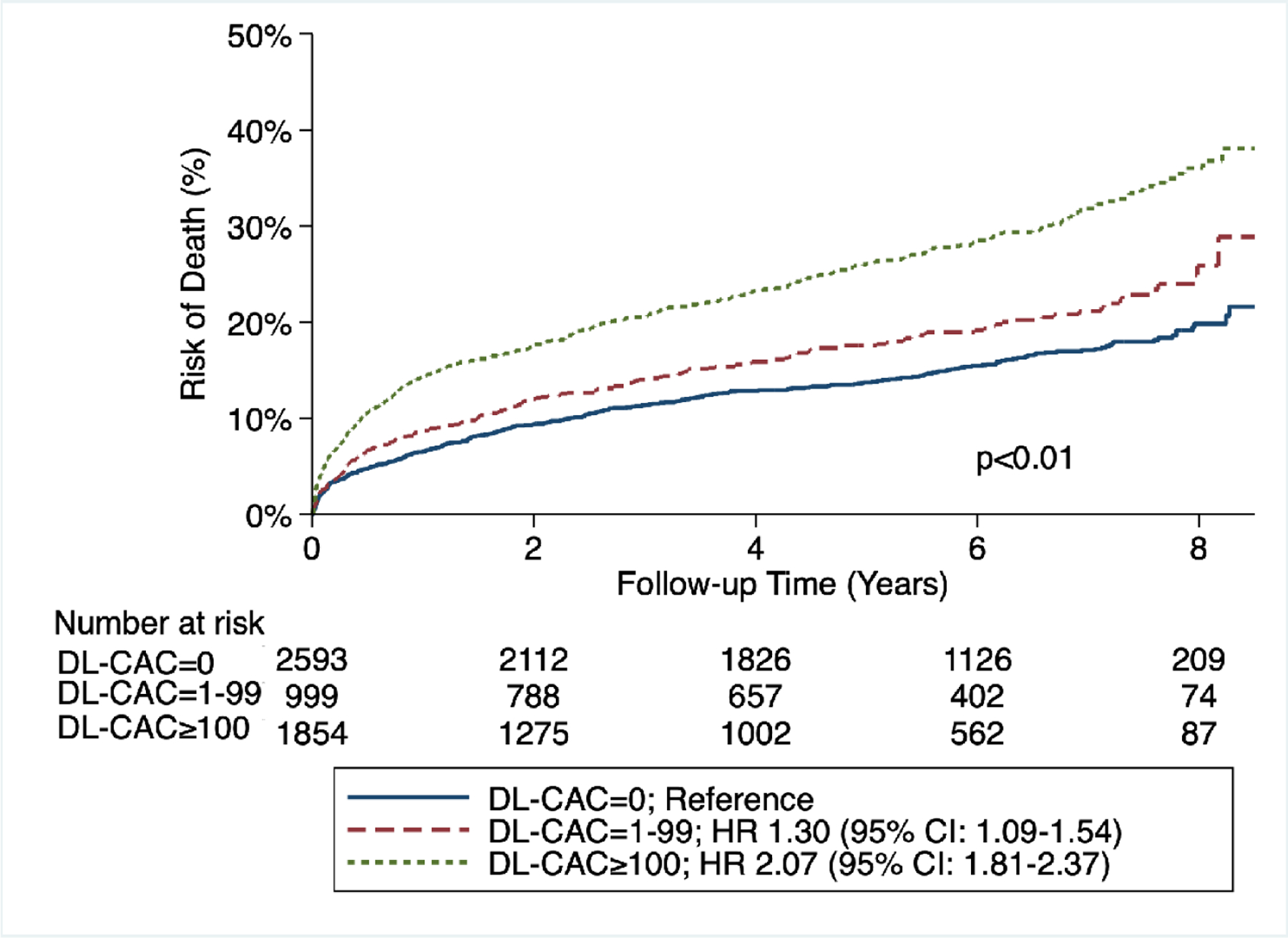
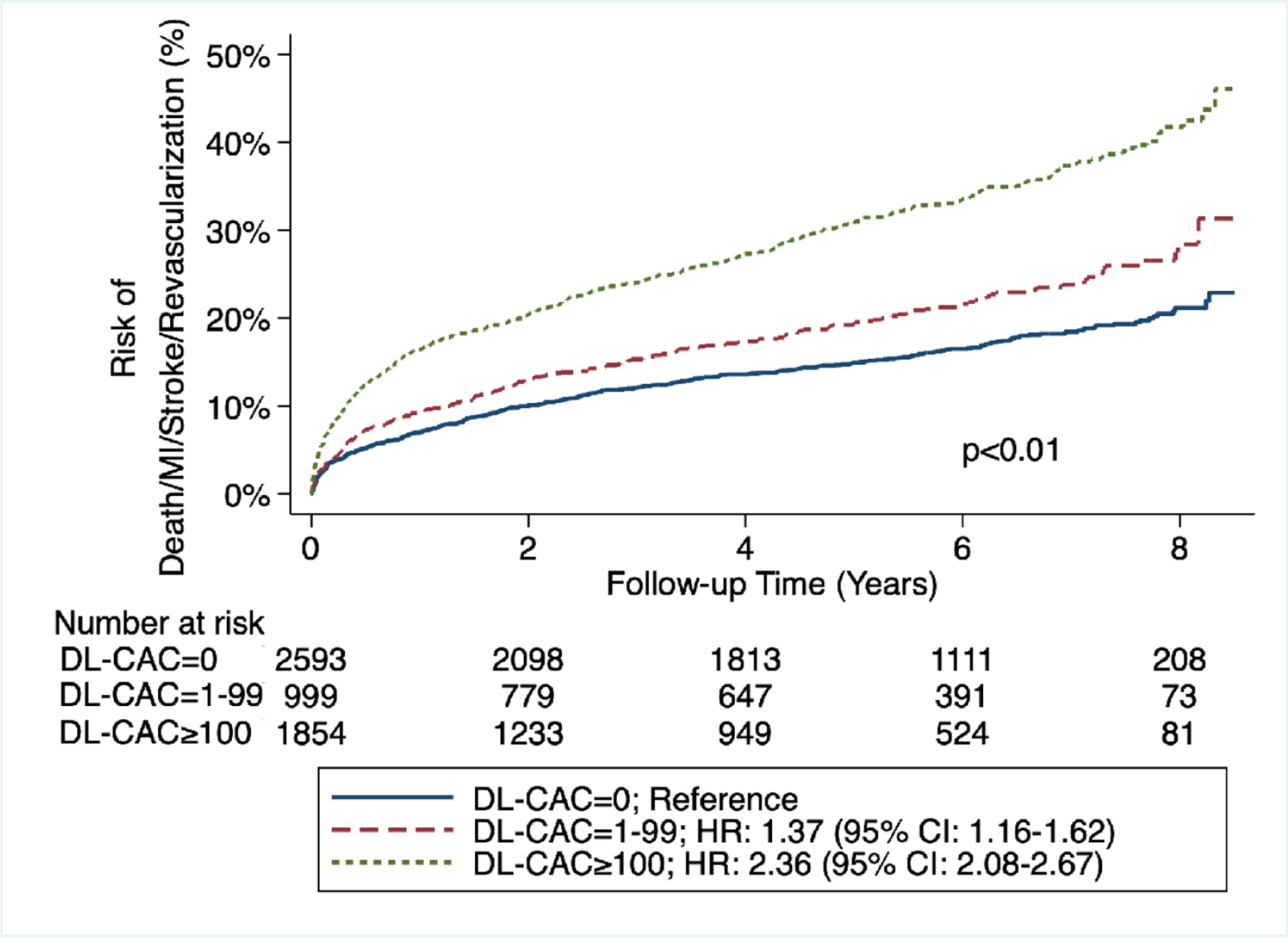
Methods: Incidental CAC was quantified using a DL algorithm (DL-CAC) on non-ECG-gated chest CTs performed for routine care in all settings at a large academic medical center from 2014 to 2019. We measured the association between DL-CAC (0, 1-99, or ≥100) with all-cause death (primary outcome), and the secondary composite outcomes of death/myocardial infarction (MI)/stroke and death/MI/stroke/revascularization using Cox regression. We adjusted for age, sex, race, ethnicity, comorbidities, systolic blood pressure, lipid levels, smoking status, and antihypertensive use. Ten-year atherosclerotic cardiovascular disease risk was calculated using the pooled cohort equations.
Results: Of 5,678 adults without ASCVD (51% women, 18% Asian, 13% Hispanic/Latinx), 52% had DL-CAC >0. Those with DL-CAC ≥100 had an average 10-year ASCVD risk of 24%; yet, only 26% were on statins. After adjustment, patients with DL-CAC ≥100 had increased risk of death (HR: 1.51; 95% CI: 1.28-1.79), death/MI/stroke (HR: 1.57; 95% CI: 1.33-1.84), and death/MI/stroke/revascularization (HR: 1.69; 95% CI: 1.45-1.98) compared with DL-CAC = 0.
Conclusions: Incidental CAC ≥100 was associated with an increased risk of all-cause death and adverse cardiovascular outcomes, beyond traditional risk factors. DL-CAC from routine non-ECG-gated CTs identifies patients at increased cardiovascular risk and holds promise as a tool for opportunistic screening to facilitate earlier intervention.
Keywords: cardiovascular outcomes; coronary artery calcium; nongated computed tomography; primary prevention; risk prediction; screening.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work was supported by the Stanford University Human-Centered Artificial Intelligence Seed Grant. Mr Khandwala and Mr Eng are employees and shareholders of Bunkerhill Health. Dr Chaudhari has received research support from the Stanford University Precision Health and Integrated Diagnostics Seed Grant and the Stanford University Human-Centered Artificial Intelligence–Artificial Intelligence in Medicine and Imaging Seed Grant; has provided consulting services to Subtle Medical, Chondrometrics GmbH, Image Analysis Group, Edge Analytics, ICM, and Culvert Engineering; is a shareholder of Subtle Medical, LVIS Corporation, and Brain Key; and receives research support from GE Healthcare and Philips, all outside of the submitted work. Dr Sandhu has received research support from the National Heart, Lung, and Blood Institute (1K23HL151672-01). Dr Rodriguez was funded by grants from the National Institutes of Health National Heart, Lung, and Blood Institute (1K01HL144607), the American Heart Association/Harold Amos Faculty Development program, and the Doris Duke Foundation (Grant #2022051); and has consulting relationships with Healthpals, Novartis, Novo Nordisk, Esperion, and AstraZeneca outside of the submitted work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


Comment in
-
Incidental Coronary Artery Calcium: Nothing Is More Expensive Than a Missed Opportunity.J Am Coll Cardiol. 2023 Sep 19;82(12):1203-1205. doi: 10.1016/j.jacc.2023.06.039. J Am Coll Cardiol. 2023. PMID: 37704310 No abstract available.
References
-
- Virani SS, Alonso A, Aparicio HJ, et al. Heart Disease and Stroke Statistics—2021 Update. Circulation. 2021;143:e254–e743. - PubMed
-
- Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364:937–952. - PubMed
-
- Peng AW, Dardari ZA, Blumenthal RS, et al. Very high coronary artery calcium (CAC ≥ 1000) and association with CVD events, non-CVD outcomes, and mortality: Results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2021:10.1161/CIRCULATIONAHA.120.050545. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
