

Thoracic Aortic Plaque Burden and Prediction of Cardiovascular Events in Patients Undergoing 320-row Multidetector CT Coronary Angiography
- PMID: 37704429
- PMCID: PMC10918031
- DOI: 10.5551/jat.64251
Thoracic Aortic Plaque Burden and Prediction of Cardiovascular Events in Patients Undergoing 320-row Multidetector CT Coronary Angiography
Abstract
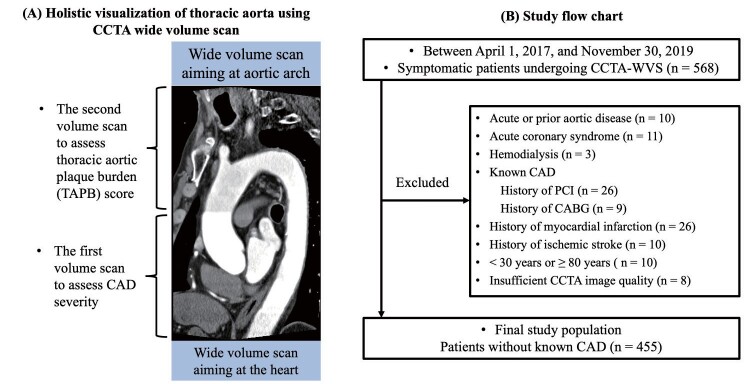
Aim: Wide volume scan (WVS) coronary computed tomography angiography (CCTA) enables aortic arch visualization. This study assessed whether the thoracic aortic plaque burden (TAPB) score can predict major cardiovascular adverse events (MACE) in addition to and independently of other obstructive coronary artery disease (CAD) attributes.
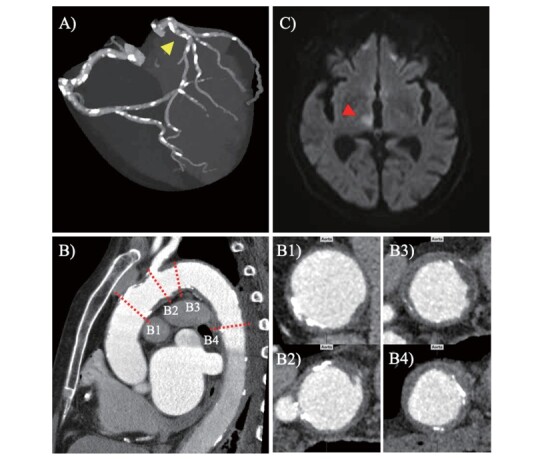
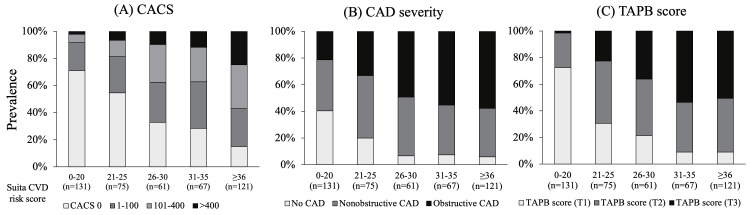
Methods: This study included patients with suspected CAD who underwent CCTA (n=455). CCTA-WVS was used to assess CAD and the prognostic capacity of TAPB scores. Data analysis included the coronary artery calcification score (CACS), CAD status and extent, and TAPB score, calculated as the sum of plaque thickness and plaque angle at five thoracic aortic segments. The primary endpoint was MACE defined as a composite event comprised of ischemic stroke, acute coronary syndrome, and cardiovascular death.
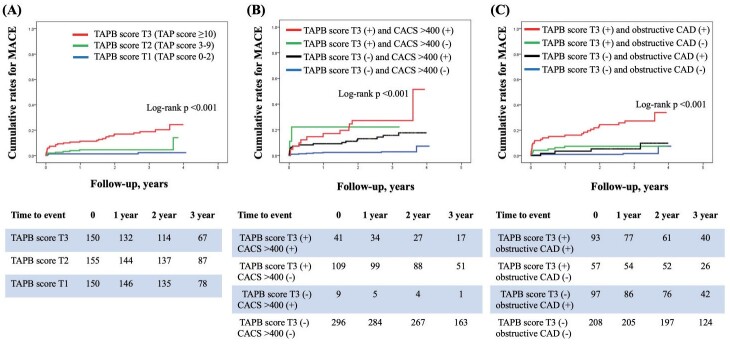
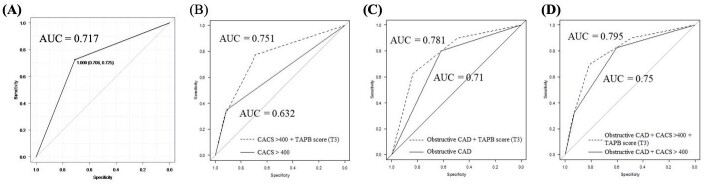
Results: During a mean follow-up period of 2.8±0.9 years, 40 of 455 (8.8%) patients experienced MACE. In the Cox proportional hazards model adjusted for clinical risks (Suita cardiovascular disease risk score), we identified TAPB score (T3) as a predictor of MACE independent of CACS >400 (hazards ratio [HR], 2.91; 95% confidence interval [CI], 1.26-6.72; p=0.012) or obstructive CAD (HR, 2.83; 95% CI, 1.30-6.18; p=0.009). The area under the curve for predicting MACE improved from 0.75 to 0.795 (p value=0.008) when TAPB score was added to CACS >400 and obstructive CAD.
Conclusions: We found that comprehensive non-invasive evaluation of TAPB and CAD has prognostic value in MACE risk stratification for suspected CAD patients undergoing CCTA.
Keywords: Atherosclerosis; Coronary artery disease; Coronary computed tomography angiography; Ischemic stroke; Prognosis.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Prognostic Value of Coronary CT Angiography for Predicting Poor Cardiac Outcome in Stroke Patients without Known Cardiac Disease or Chest Pain: The Assessment of Coronary Artery Disease in Stroke Patients Study.Korean J Radiol. 2020 Sep;21(9):1055-1064. doi: 10.3348/kjr.2020.0103. Korean J Radiol. 2020. PMID: 32691541 Free PMC article.
-
Aortic arch plaque morphology in patients with coronary artery disease undergoing coronary computed tomography angiography with wide-volume scan.Coron Artery Dis. 2022 Nov 1;33(7):531-539. doi: 10.1097/MCA.0000000000001171. Epub 2022 Jul 22. Coron Artery Dis. 2022. PMID: 35866499 Free PMC article.
-
[Value of fractional flow reserve derived from coronary computed tomographic angiography and plaque quantitative analysis in predicting adverse outcomes of non-obstructive coronary heart disease].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Jun;35(6):615-619. doi: 10.3760/cma.j.cn121430-20230215-00092. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37366128 Chinese.
-
Atherosclerosis evaluation and cardiovascular risk estimation using coronary computed tomography angiography.Eur Heart J. 2024 May 27;45(20):1783-1800. doi: 10.1093/eurheartj/ehae190. Eur Heart J. 2024. PMID: 38606889 Free PMC article. Review.
-
[Plaque characterization and individualized risk assessment].Radiologie (Heidelb). 2024 Dec;64(12):946-955. doi: 10.1007/s00117-024-01385-y. Epub 2024 Nov 12. Radiologie (Heidelb). 2024. PMID: 39532741 Free PMC article. Review. German.
Cited by
-
Prevalence of ascending aortic atheromatous plaques and risk factors in Thai cardiac surgery patients: A prospective cohort study.Heliyon. 2024 Aug 21;10(16):e36607. doi: 10.1016/j.heliyon.2024.e36607. eCollection 2024 Aug 30. Heliyon. 2024. PMID: 39262997 Free PMC article.
-
Onset and progression of atherosclerosis in patients with melanoma treated with immune checkpoint inhibitors.J Immunother Cancer. 2025 Apr 24;13(4):e011226. doi: 10.1136/jitc-2024-011226. J Immunother Cancer. 2025. PMID: 40280566 Free PMC article.
-
Aortic Arch Calcification in Predicting Unfavorable Angiographic Outcomes for Patients with ST-Elevation Myocardial Infarction Undergoing Percutaneous Coronary Intervention.Med Princ Pract. 2024;33(6):587-596. doi: 10.1159/000540026. Epub 2024 Jun 26. Med Princ Pract. 2024. PMID: 38934156 Free PMC article.
-
The research progress and research trends in acute coronary syndrome nursing: A review of visual analysis based on the Web of Science database.Medicine (Baltimore). 2024 Feb 16;103(7):e35849. doi: 10.1097/MD.0000000000035849. Medicine (Baltimore). 2024. PMID: 38363951 Free PMC article. Review.
-
Impact of epicardial adipose tissue on diastolic dysfunction in patients with chronic coronary syndrome and preserved left ventricular ejection fraction.Eur Heart J Imaging Methods Pract. 2024 Jun 5;2(1):qyae056. doi: 10.1093/ehjimp/qyae056. eCollection 2024 Jan. Eur Heart J Imaging Methods Pract. 2024. PMID: 39224094 Free PMC article.
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Shay CM, Spartano NL, Stokes A, Tirschwell DL, VanWagner LB, Tsao CW. Heart disease and stroke statistics—2020 update: A report from the American Heart Association. Circulation, 2020; 141: e139-596 - PubMed
-
- Yasuda S, Miyamoto Y, Ogawa H. Current Status of Cardiovascular Medicine in the Aging Society of Japan. Circulation, 2018; 138: 965-967 - PubMed
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J, 2020; 41: 407-477 - PubMed